["17f64572023d9d92f9a68047fd52e1e660e1bf8d","d47466d1294abb83933ea7ddb79b56d460b55e40"]
Breast reduction
breast
reduction
macromastia
hypertrophy
ptosis
6895
6895
Chapter reads
0
0
Chapter likes
9/10
Evidence score
14
14
Images included
07
7
Videos included
01
Anatomy and Classification of Surgical Techniques
Introduction
After reading this chapter, the participant should be able to:
1. Understand the different techniques of breast reduction based on the anatomy of both the vascular supply and the Innervation of the breast.
2. Identify the most appropriate technique for each patient using our algorithm.
3. Optimize pre- and postoperative care to provide consistent predictable results in breast reduction.
1. Understand the different techniques of breast reduction based on the anatomy of both the vascular supply and the Innervation of the breast.
2. Identify the most appropriate technique for each patient using our algorithm.
3. Optimize pre- and postoperative care to provide consistent predictable results in breast reduction.
Surgical anatomy26
Vascular supply
Arterial and venous supply follow the same pattern. Breast parenchyma and skin are supplied by:
- perforating branches of internal mammary artery
- lateral thoracic artery
- thoracodorsal artery
- intercostal perforators
- thoracoacromial artery.
Blood supply to the breast consists of a deep artery and vein that course up into the parenchyma from the fourth interspace. The rest of the blood supply (mainly from the internal mammary system) comes up around the breast periphery and then courses toward the nipple in the subcutaneous tissue covering the breast. The veins travel just deep to the dermis, and the majority of them course superomedially. 2427
- perforating branches of internal mammary artery
- lateral thoracic artery
- thoracodorsal artery
- intercostal perforators
- thoracoacromial artery.
Blood supply to the breast consists of a deep artery and vein that course up into the parenchyma from the fourth interspace. The rest of the blood supply (mainly from the internal mammary system) comes up around the breast periphery and then courses toward the nipple in the subcutaneous tissue covering the breast. The veins travel just deep to the dermis, and the majority of them course superomedially. 2427
Innervation4
The nipple is mainly innervated by the anterior branch of the lateral fourth intercostal nerve. There is a superficial branch that has to be sacrified in all types of pedicle but the lateral. The deep branch that courses over the pectoralis muscle can be preserved by chosing a medial or inferior full-thickness pedicle. Additional various smaller branches arise medial from the second, third and fourth intercostal space, also providing innervation of the nipple.24
Fibrous tissue of the gland
The mammary gland is located in the region of the 3rd to 6th rib (anatomical variation possible). It sits on the pectoralis major muscle, whose fascia forms the separating layer between the muscle and the glandular tissue. The glandular tissue of the breast consists of 15-20 lobes, which can be divided into smaller lobules. The glandular ducts run through the breast parenchyma, which merge into the excretory ducts and finally flow into the sinus lactiferi below the nipple. The nipple, also called papilla mammae, is characterized by a conical shape and is surrounded by the pigmented areola mammae 28. The nipple and areola together are often summarized in the literature and also in this work as the nipple-areola complex (NAC)29.According to Prantl et al 30, the breast has a complex fascial system consisting of a superficial and a deep fascial sheet. The former divides into an anterior and posterior leaflet at the level of the first rib. The posterior sheet, together with the muscle fascia of the pectoralis major muscle, separates the glandular tissue from the muscle and forms a sliding bearing. From the aforementioned muscle fascia also arise the so-called Cooper ligaments, which run horizontally through the breast and end in the dermis 30. Along the Cooper ligaments also run the blood and lymph vessels, as well as the nerve conduction pathways from the depths to the central area of the nipple 28.The anterior superficial fascial sheet exists only in the cranial region of the breast and extends approximately to the 4th intercostal space 30. The peculiarity of the female breast is its strong displaceability. This is due to the fact that the superficial and deep breast fasciae do not serve to attach the breast itself, but merely envelop the mamma . The triangular complex contributes to the stabilization of the inframammary fold. This consists of the muscle septa of musculus rectus abdominis, musculus pectoralis major and the fifth rib. Clavicular ligaments support the cranial mamma. In addition, there is a radial ligament system that lies annularly around the glandular tissue and stabilizes it .An important anatomic structure for surgery is the Würinger's septum. It contains the central blood supply to the mamma, thereby allowing safe styletization of the breast and NAC. The Würinger's septum is a fascial structure that contains the main branch of the arteria thoracica interna to supply blood to the breast 29. It arises from the pectoral muscle fascia, runs to the nipple at the level of the 5th rib according to Würinger et al 31, and also contains the main nerve supply to the nipple 31.Phenotypically, Würinger's septum is characterized by great anatomic variation. The expression of the vessels ranges from central, powerful vessels to several delicate vessels, which usually run over the 5th rib. As a result, the Würinger's septum is often hard to identifiy. This is probably also the reason why this important and surgically relevant structure was not described until 1998 by the eponym Elisabeth Würinger et al.
Classification of surgical techniques
Pedicle selection
Inferior pedicle
The inferior pedicle has been the preferred method (in the United States) and is easily teachable. The NAC is maintained on an inferior dermal- parenchymal pedicle. Usually paired with an inverted-T skin excision.
Disadvantages: When the distance between nipple to inframammary fold is >18 cm, the pedicle tend to become bulky. This can limit the extent of reduction and can lead to a boxy shape of the breast with pseudoptosis.
Advantages: Easy to teach.
Disadvantages: When the distance between nipple to inframammary fold is >18 cm, the pedicle tend to become bulky. This can limit the extent of reduction and can lead to a boxy shape of the breast with pseudoptosis.
Advantages: Easy to teach.
Cranial/mediocranial pedicle
NAC is maintained on a cranial or mediocranial dermal-parenchymal pedicle. Lassus is credited with introduction of the cranial pedicle technique wich was then refined by Lejour. Hall-Findlay popularized the mediocranial pedicle..
Advantages: The big advantage of this method is that the pedicle is located cranial, where volume is commonly desired. Moreover it allows creation of an inferior pillar support to limit pseudoptosis and provides a very safe perfusion of the NAC.
"A true supero medial pedicle has a dual axial blood supply that increases safety: the second and the third superficial branch of the internal mammary artery"27
Advantages: The big advantage of this method is that the pedicle is located cranial, where volume is commonly desired. Moreover it allows creation of an inferior pillar support to limit pseudoptosis and provides a very safe perfusion of the NAC.
"A true supero medial pedicle has a dual axial blood supply that increases safety: the second and the third superficial branch of the internal mammary artery"27
Central mound technique
The NAC is maintained on a central parenchymal pedicle (without dermis).
Disadvantages: This pedicle is less reliable for NAC neurovascular supply.
Advantages: Allows variable resection of parenchyma in multiple quadrants.
Disadvantages: This pedicle is less reliable for NAC neurovascular supply.
Advantages: Allows variable resection of parenchyma in multiple quadrants.
Skin resection pattern
Vertical pattern
The vertical scar allows excision of lax skin in horizontal dimension.
We use temporary staples as tailor tacking to facilitate incision placement. Once desired shape and skin contour are obtained, the “tailored” resection pattern is marked and excised.(video). We avoid a transverse scar by gathering the skin in the vertical closure. (shorten the vertical scar with double intracutaneous suture).
We use temporary staples as tailor tacking to facilitate incision placement. Once desired shape and skin contour are obtained, the “tailored” resection pattern is marked and excised.(video). We avoid a transverse scar by gathering the skin in the vertical closure. (shorten the vertical scar with double intracutaneous suture).
Inverted T pattern
Skin excision includes both a vertical and horizontal excision: Horizontal skin excess is removed through the vertical incision. Vertical skin excess is removed with the horizontal excision placed in the inframammary fold (IMF).
Advantages: This technique is useful in large reductions with excessive amounts of skin redundancy.
Disadvantages: It can lead to wound healing problems at the intersection point in the IMF.
Advantages: This technique is useful in large reductions with excessive amounts of skin redundancy.
Disadvantages: It can lead to wound healing problems at the intersection point in the IMF.
Horizontal pattern
The horizontal scar reduction mammoplasty is a safe and reliable method of reduction mammaplasty when there is macromasty and significant ptosis.
Advantages:This technique avoids the vertical scar and hides the transverse scar in the inframammary fold.
Advantages:This technique avoids the vertical scar and hides the transverse scar in the inframammary fold.
02
Metrics and Volumetry of the Breast
Metrics and Volumetry of the Breast
The ideal breast shape
Beauty is in the eye of the beholder1415. In an experimental study on female bodily attractiveness (varying weight, bust size, waist width, hip width and leg length independently) we could even prove that males prefer a larger bust size in women than females themselves10.
Nevertheless, it seems fundamental to define and objectively measures of the breast for surgical planning and for evaluation of surgical outcome16.
The definition of the ideal breast is commonly symmetric. Even if symmetry naturally does not exist19.
The ideal NAC position is located at the point of maximal projection of the breast. It should be in the middle of the breast mound vertically and slightly lateral to the meridian horizontally (40:60)13. Mallucci describes that 55% of the breast volume should be below the NAC and 45% above it1720.
Nevertheless, it seems fundamental to define and objectively measures of the breast for surgical planning and for evaluation of surgical outcome16.
The definition of the ideal breast is commonly symmetric. Even if symmetry naturally does not exist19.
The ideal NAC position is located at the point of maximal projection of the breast. It should be in the middle of the breast mound vertically and slightly lateral to the meridian horizontally (40:60)13. Mallucci describes that 55% of the breast volume should be below the NAC and 45% above it1720.
Volumetry
Together with ReMIC (Regensburg Medical Image Computing), we founded in Regensburg the DPS (Digital Plastic Surgery Research Group), we are dedicated to evaluate and develop 3D Models of the body, specifically the breast. (see Chapter 3D in PlastiCademy). We developed a novel digital method of outcome assessment in breast surgery12..Indeed three-dimensional body surface imaging is adequate for volume approximation23. If 3D assessment is not possible, then linear measurements are reliable. From different mathematical formulas proposed for the calculation of breast volume we use the Breast V, because of its accuracy and practicability2122.
Glossar of standard landmarks
SN= sternal notch
N= nipple
MC= mid-clavicle
ML=midline
F= inframammary fold
Fp= inframammary fold projection
A= top edge of the areola
FFp= distance between the inframammary fold and the ventral projection of the inframammary fold
NF=distance between the nipple and the inframammary fold
NFp= distance between the nipple and the ventral projection of the inframammary fold
AFP= distance between the top Edge of the areola and the ventral projection of the inframammary fold
N= nipple
MC= mid-clavicle
ML=midline
F= inframammary fold
Fp= inframammary fold projection
A= top edge of the areola
FFp= distance between the inframammary fold and the ventral projection of the inframammary fold
NF=distance between the nipple and the inframammary fold
NFp= distance between the nipple and the ventral projection of the inframammary fold
AFP= distance between the top Edge of the areola and the ventral projection of the inframammary fold
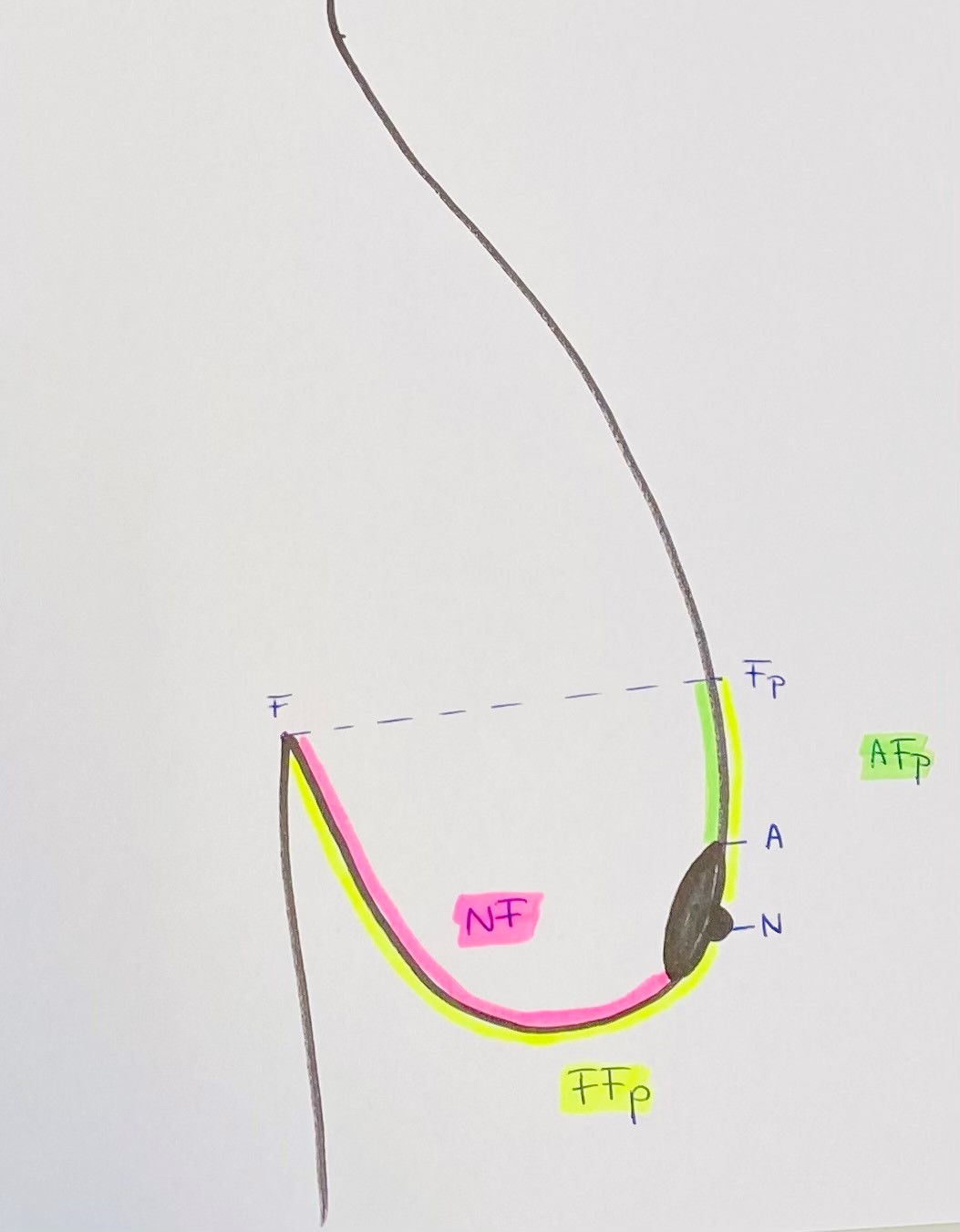
linear measures of the breast
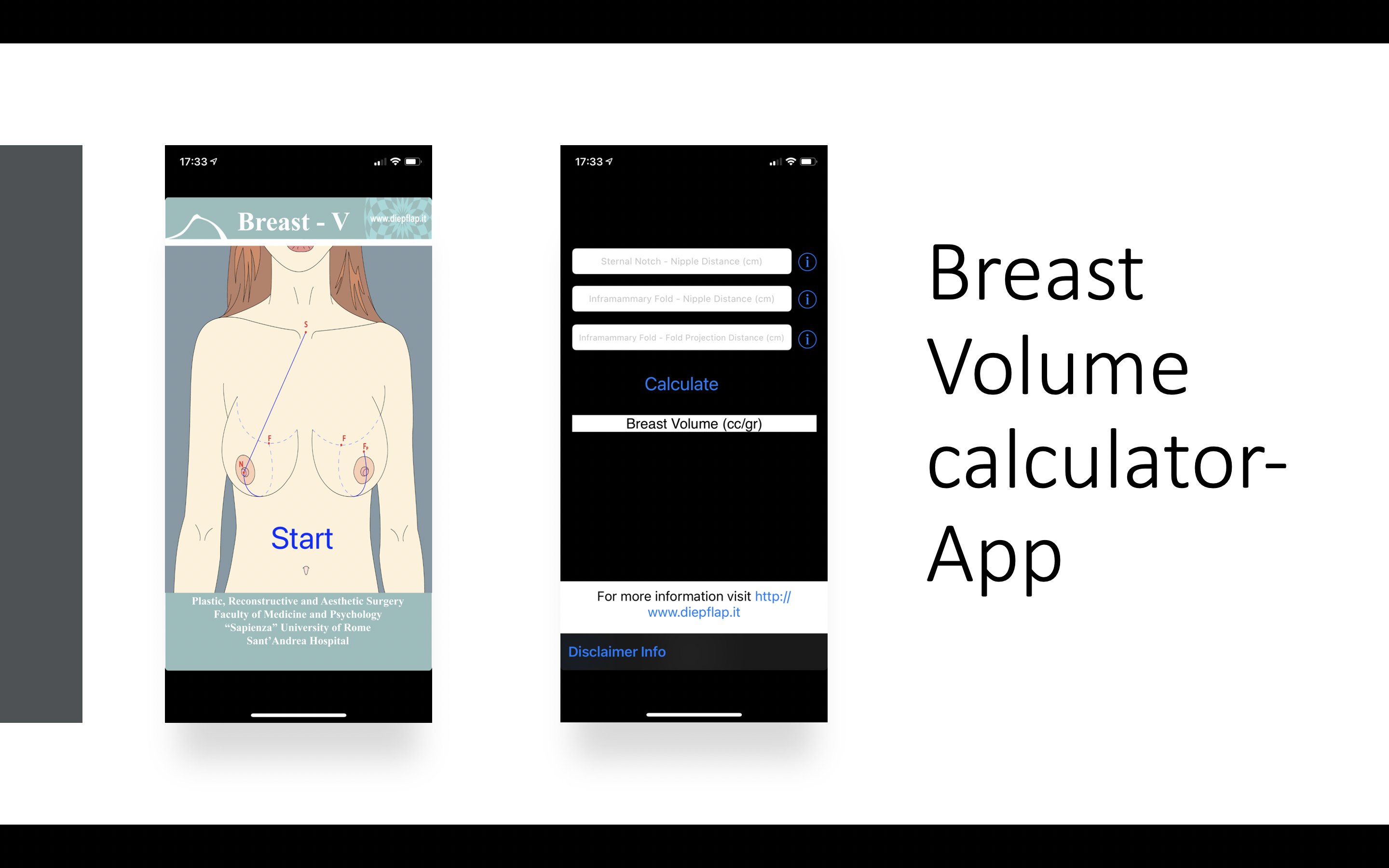
Breast Volume calculator
03
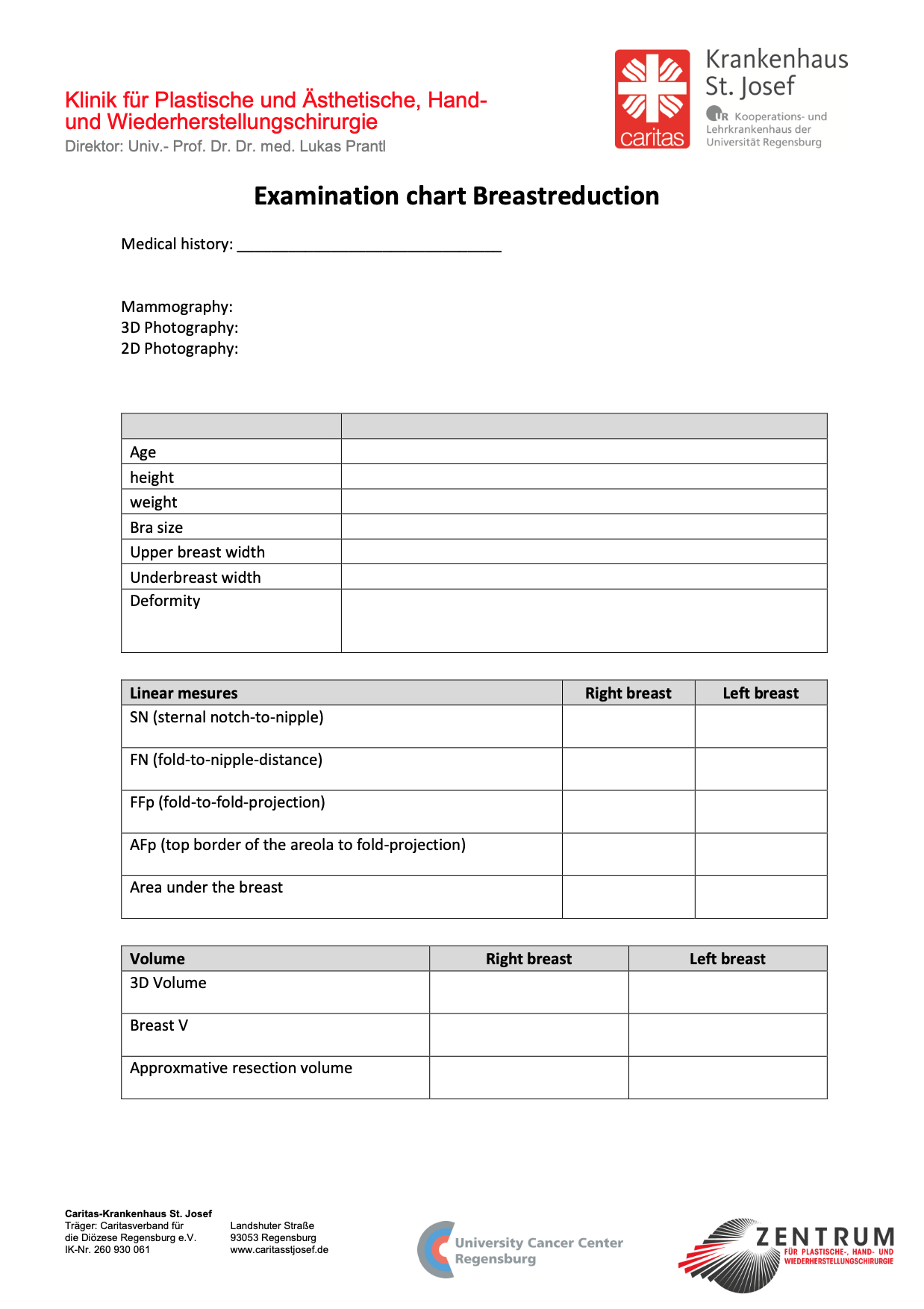
Examination
04
Algorithm
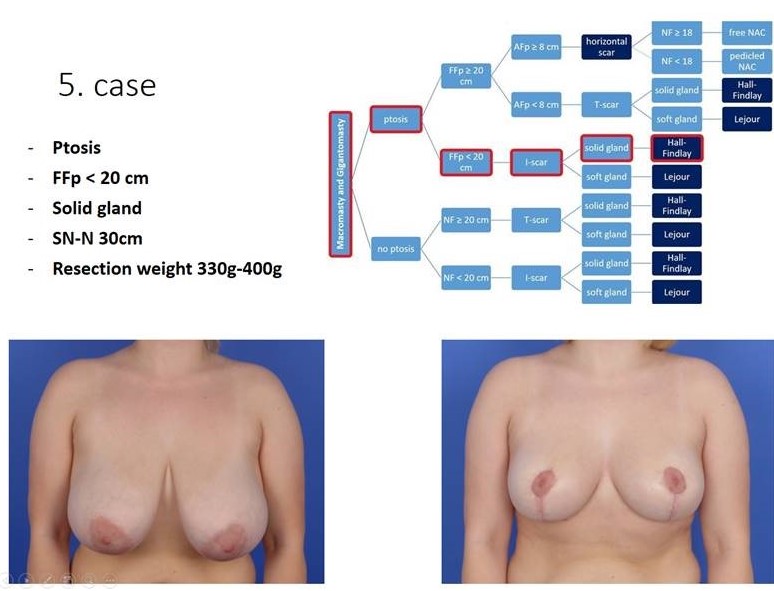
Algorithm flow chart
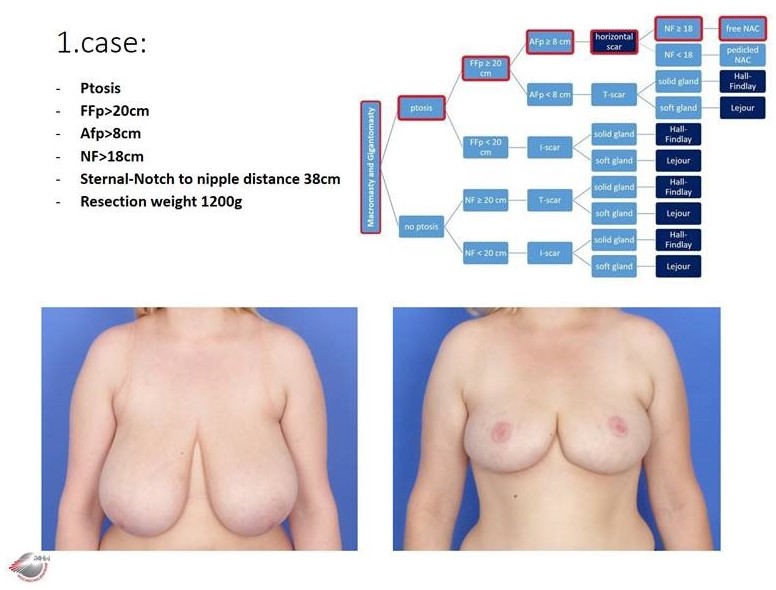
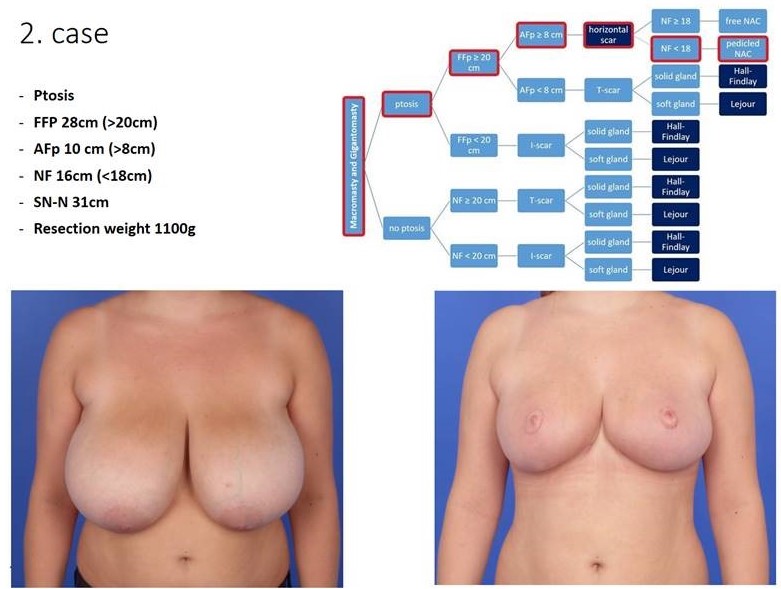
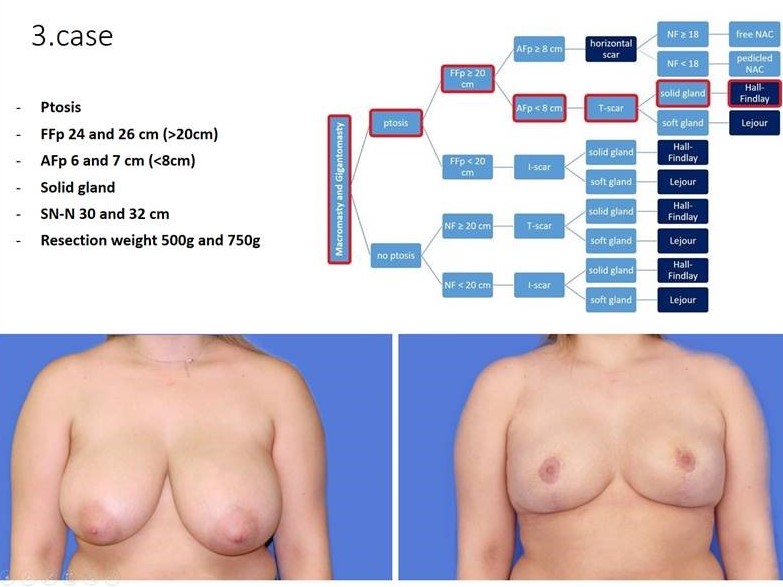
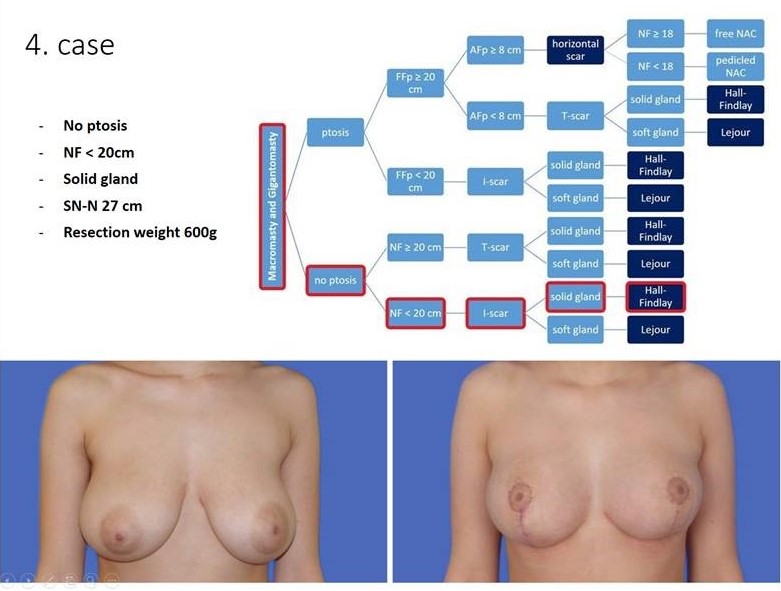
The extend of macromastia is described by the preoperative linear measures described before and used for the Breast-V21. Depending on the extend of macromastia, we use different techniques. Through retrospective anlaysis we developed a algorithm for chosing the optimal skin reduction pattern, technique of glandular resection and type of pedicle, regardig the measurements as described below.
The first decisional criterion of our algorithm is the ptosis mammae. If the nipple is above the submammary fold, there is no ptosis and less skin excess. In this case it is not necessary to have extensive skin resection.
If there is a ptosis the second decisional criterion of our algorithm is the distance between the inframammary fold and the fold projection (FFp). The fold projection correlates with the new position of the NAC after reduction mammoplasty. If FFp is longer than 20cm, we will have an extensive skin excess and need an inverted T or horizontal scar for appropriate reduction. Otherwise we can chose a vertical pattern leading to an I-shaped scar.
To decide if we can chose the horizontal scar the third decisional criterion is the distance between the new position of the NAC and the upper edge of the areola (AFP). If this distance is 8 cm or above we can perform a horizontal scar reduction.
The fourth criterion is the distance between the fold and the nipple. If this distance is more than 18cm, we prefer a free NAC graft. (weak vascularity of the inferior-central pedicle)
Beside those criteria, we prefer a cranial pedicle (Lejour) for a soft gland and a mediocranial pedicle (Hall-Findlay) for a solid gland. A solid gland is easier to rotate than to translate.
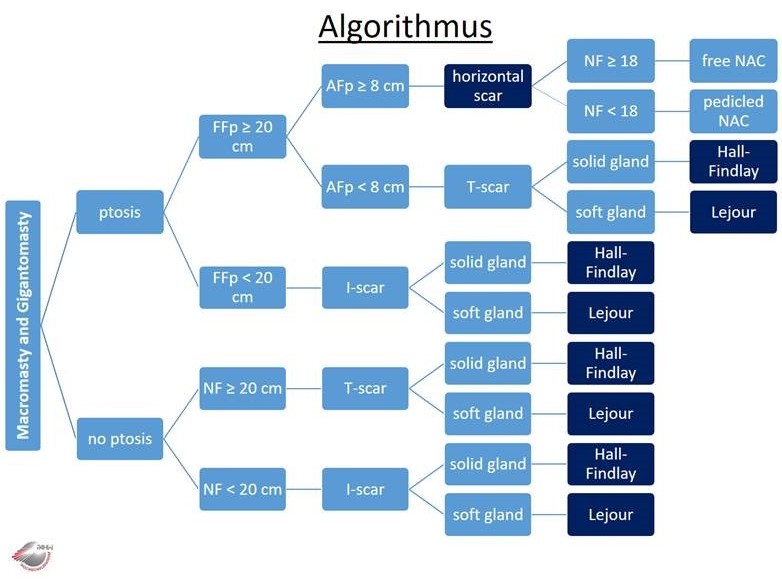
Treatment Algorithm for Breast Reduction
Appliance of the algorithm
horizontal scar, free NAC
horizontal scar, pedicled NAC
T scar, Hall-Findlay (mediocranial pedicle)
vertical scar, Hall-Findlay (mediocranial)
vertical scar, Hall-Findlay (mediocranial pedicle)
05
Preoperative Markings and Surgical Technique of Superomedial Pedicled Breast Reduction
Mediocranial Pedicled Breast Reduction24
We combine the mediocranial pedicle with a non resorbable pexy of the gland to the pectoralis fascia (modified Hall-Findlay).
When the breast is less ptotic, we perform a vertical scar breast reduction (I-scar). If the breast is more ptotic, we need a short inverted T scar, which is marked at the end of surgery after tailor tacking the horizontal part of the scar. In order to prevent distortion of the NAC and widening of the periareolar scar, we perform a periareolar resorbable suture. First it was a purse string suture, then we changed to a wheel suture. Latest we tend to use a net suture. The net suture prevents not only the distortion of the NAC but also a bulging of the NAC. The net suture is demonstrated in the video below.
To prevent a "boxy shape" of the breast, the T-spot of the inverted T-scar has to be the lowest point of the scar.
When the breast is less ptotic, we perform a vertical scar breast reduction (I-scar). If the breast is more ptotic, we need a short inverted T scar, which is marked at the end of surgery after tailor tacking the horizontal part of the scar. In order to prevent distortion of the NAC and widening of the periareolar scar, we perform a periareolar resorbable suture. First it was a purse string suture, then we changed to a wheel suture. Latest we tend to use a net suture. The net suture prevents not only the distortion of the NAC but also a bulging of the NAC. The net suture is demonstrated in the video below.
To prevent a "boxy shape" of the breast, the T-spot of the inverted T-scar has to be the lowest point of the scar.
Preoperative Markings 13
Surgical Technique
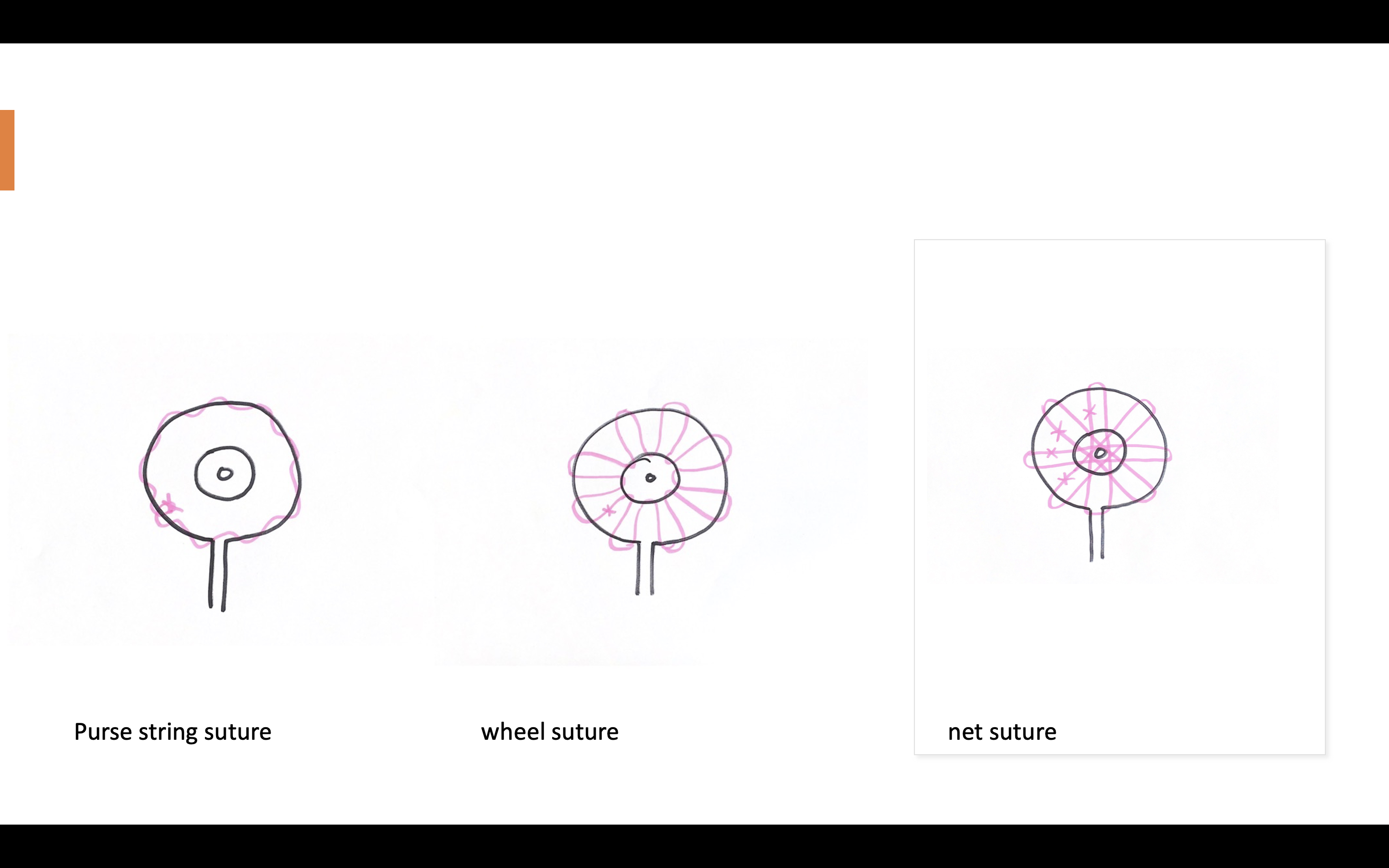
periareolar suture
inverted T
06
Preoperative Markings and surgical Technique of Inferior-central Pedicled Breast Reduction and Horizontal Scar
Inferior-central Pedicled Breast Reduction and Horizontal Scar
Preoperative Markings
Surgical Technique
We use to perform vertical scar reduction mammoplasty even on gigantomasty13.We were not satisfied with shape (disfiguring pull of the vertical limb on the shape of the new areola) and bad scarring so we changed . First we changed for the inferior pedicle and inverted T Scar. Because of healing complications of the inferior T- connection on a standard wise pattern, we decide to perform the horizontal scar mammoplasty on gigantomastia. This technique has been described bei Passot 192538, Lalonde a couple of years later 39. Ribeiro described it in 1975 as a new technique40. The horizontal scar reduction mammoplasty is a safe and reliable method of reduction mammaplasty when there is macromasty and significant ptosis. We use it with a wide inferior central pedicle. This technique avoids the vertical scar and hides the transverse scar in the shadow of the inferior breast. We use it with two slight modifications: The horizontal scar has to be laterally nearly vertical in order to remove the preaxillary skin excess. The deepithelized inferior pedicle is shaped like in Rubins mastopexy technique for massive weight losers and works as an "inner bra".
Free nipple graft and modified horizontal scar with inferior-central flap40
Surgical Technique
07
Evidence based perioperative Management
Evidence based perioperative management25
Preoperative Imaging7
Evidence supports the concept that the decision to perform a preoperative mammogram should be individualized by the patients family history of breast cancer, genetic testing results, evidence of mass on clinical examination and the age of the individual. Every patient older then 50 years should have a recent mammogram, and many believe that those older than 40 years should do as well.25
Perioperative antibiotics
No evidence. We do give single shot antibiotics Cefalosporine 1. Generation
Breast infiltration
The use of a dilute epinephrine wetting agent injected along the incision lines before commencement of the breast reduction has demonstrated a reduction in the amount of blood loss. The review of Kerrigan and Slezak ( 6271 patients included) could prove that the intraoperative use of epinephrine doesn't increase the risk of postoperative hematoma. 35
Deep venous thrombosis prophylaxis
In a Review of 17774 plastic surgery patients, Wes et al found 46 patients with deep vein thrombosis and 44 with pulmonary emboli, for an overall rate of 0,51 %37 Older patients with obesity and lack of mobility have a higher risk of thromboembolism and need beside pneumatic compression boots during and after surgery a low molecular weight heparin.
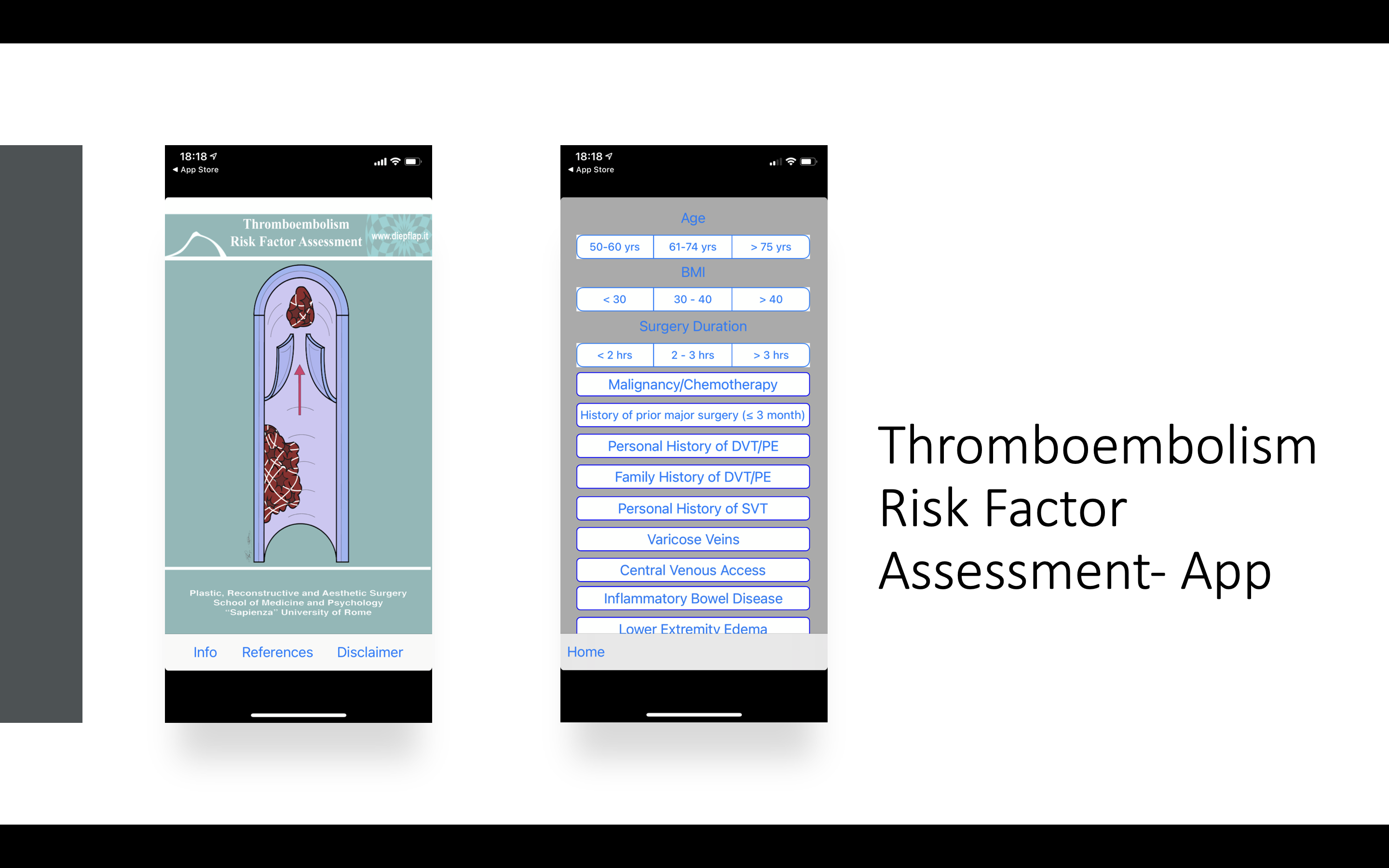
Thromboembolism Risk Factor Assessment-App
Postoperative drains6
Many studies have demonstrated that postoperative use of drains has led to no difference in hematoma rates, no difference in wound healing complications and greater patient discomfort.
Images
linear measures of the breast
examination chart
inverted T
periareolar suture
algorithm
Breast V App
Breast Volume calculator
Thromboembolism Risk Factor Assessment-App
Treatment Algorithm for Breast Reduction
horizontal scar, free NAC
horizontal scar, pedicled NAC
T scar, Hall-Findlay (mediocranial pedicle)
vertical scar, Hall-Findlay (mediocranial pedicle)
vertical scar, Hall-Findlay (mediocranial)
Videos
supermedial pedicle-inverted T scar- modified Hall Findlay
Breast reduction modified Hall Findlay, T-scar, superomedial pedicle
Breast reduction horizontal scar, inferocentral pedicle
markings Breast reduction horizontal scar
Metrics of the Breast
Markings modified Hall-Findlay
Breast Reduction with free nipple graft, inferior central flap and horizontal scar
References
[1]
Essentials of Aesthetic Surgery, Jeffrey E.Janis, Thieme, 2018
[2]
Breast Reduction, Hall-Findlay Elizabeth J., Shestak Kenneth C., Ovid Technologies (Wolters Kluwer Health), 2015
[3]
Discussion: The Blood Supply of the Breast Revisted, Hall-Findlay Elizabeth J., Ovid Technologies (Wolters Kluwer Health), 2016
[4]
Breast sensitivity after mastectomy and autologous reconstruction, Heine Norbert, Koch Christoph, Brebant Vanessa, Kehrer Andreas, Anker Alexandra, Prantl Lukas, IOS Press, 2017
[5]
Breast Reduction, Hall-Findlay Elizabeth J., Shestak Kenneth C., Ovid Technologies (Wolters Kluwer Health), 2015
[6]
Plastische und rekonstruktive Chirurgie der Brust. 2., komplett aktualisierte Auflage, Gabka CJ, Bohmert H, Blondeel P, Gabka-Bohmert. , Stuttgart: Georg Thieme Verlag; 2006. S. 281, 2006
[7]
Chirurgische Anatomie. In: Brustchirurgie , Fansa H, Heitmann C. , Berlin Heidelberg: Springer-Verlag; 2018, 2018
[8]
Die tuberöse Brustdeformität- ein Behandlungsalgorithmus, Prantl L, Wenzel C, Heine N, Brix E, Brébant V. , Plast Chir. 19(4):191–200., 2019
[9]
Die tuberöse Brustdeformität- ein Behandlungsalgorithmus, Prantl L, Wenzel C, Heine N, Brix E, Brébant V. , Plast Chir. 19(4):191–200., 2019
[10]
Plastische und rekonstruktive Chirurgie der Brust. 2., komplett aktualisierte Auflage, Gabka CJ, Bohmert H, Blondeel P, Gabka-Bohmert. , Stuttgart: Georg Thieme Verlag; 2006. S. 281, 2006
[11]
Die tuberöse Brustdeformität- ein Behandlungsalgorithmus, Prantl L, Wenzel C, Heine N, Brix E, Brébant V. , Plast Chir. 19(4):191–200., 2019
[12]
Chirurgische Anatomie. In: Brustchirurgie , Fansa H, Heitmann C. , Berlin Heidelberg: Springer-Verlag; 2018, 2018
[13]
Nerve and Vessel Supplying Ligamentous Suspension of the Mammary Gland, Würinger E, Mader N, Posch E, Holle J, Plast Reconstr Surg. Mai 1998;101(6):1486–1493., 1998
[14]
Nerve and Vessel Supplying Ligamentous Suspension of the Mammary Gland, Würinger E, Mader N, Posch E, Holle J, Plast Reconstr Surg. Mai 1998;101(6):1486–1493., 1998
[15]
Discussion: The Blood Supply of the Breast Revisted, Hall-Findlay Elizabeth J., Ovid Technologies (Wolters Kluwer Health), 2016
[16]
Aesthetic Breast Shape Preferences Among Plastic Surgeons, Broer Peter Niclas, Juran Sabrina, Walker Marc E., Ng Reuben, Weichman Katie, Tanna Neil, Liu Yuen-Jong, Shah Ajul, Patel Anup, Persing John A., Thomson James Grant, Ovid Technologies (Wolters Kluwer Health), 2015
[17]
Ideal Anthropomorphic Values of the Female Breast, Liu Yuen-Jong, Thomson James G., Ovid Technologies (Wolters Kluwer Health), 2011
[18]
Males Prefer a Larger Bust Size in Women Than Females Themselves: An Experimental Study on Female Bodily Attractiveness with Varying Weight, Bust Size, Waist Width, Hip Width, and Leg Length Independently, Prantl Lukas, Gründl Martin, Springer Science and Business Media LLC, 2011
[19]
Anthropomorphic Breast Measurement: Protocol and Results in 50 Women with Aesthetically Perfect Breasts and Clinical Application, Westreich Melvyn, Ovid Technologies (Wolters Kluwer Health), 1997
[20]
BFACE, Martinovic Maryann E., Blanchet Nadia P., Ovid Technologies (Wolters Kluwer Health), 2017
[21]
The Aesthetically Ideal Position of the Nipple–Areola Complex on the Breast, Lewin Richard, Amoroso Matteo, Plate Nikolina, Trogen Clara, Selvaggi Gennaro, Springer Science and Business Media LLC, 2016
[22]
Shapes, Proportions, and Variations in Breast Aesthetic Ideals, Mallucci Patrick, Branford Olivier Alexandre, Elsevier BV, 2015
[23]
Metrics of the Aesthetically Perfect Breast, Atiye Bishara, Chahine Fadel, Springer Science and Business Media LLC, 2018
[24]
The notion of the ideal breast and its variability: Reviewing the difficulty of perceiving beauty through defined margins, Rubano Amanda, Siotos Charalampos, Rosson Gedge D., Manahan Michele A., Wiley, 2019
[25]
Preoperative breast volume evaluation of one-stage immediate breast reconstruction using three-dimensional surface imaging and a printed mold, Chen Keng, Feng Chin-Jung, Ma Hsu, Hsiao Fu-Yin, Tseng Ling-Ming, Tsai Yi-Fang, Lin Yen-Shu, Huang Li-Ying, Yu Wen-Chan, Perng Cherng-Kang, Ovid Technologies (Wolters Kluwer Health), 2019
[26]
The BREAST-V, Longo Benedetto, Farcomeni Alessio, Ferri Germano, Campanale Antonella, Sorotos Micheal, Santanelli Fabio, Ovid Technologies (Wolters Kluwer Health), 2013
[27]
A prospective study of breast anthropomorphic measurements, volume and ptosis in 605 Asian patients with breast cancer or benign breast disease, Huang Nai-si, Quan Chen-lian, Mo Miao, Chen Jia-jian, Yang Ben-long, Huang Xiao-yan, Wu Jiong, Public Library of Science (PLoS),
[28]
Chirurgische Anatomie. In: Brustchirurgie , Fansa H, Heitmann C. , Berlin Heidelberg: Springer-Verlag; 2018, 2018
[29]
Die tuberöse Brustdeformität- ein Behandlungsalgorithmus, Prantl L, Wenzel C, Heine N, Brix E, Brébant V. , Plast Chir. 19(4):191–200., 2019
[30]
The BREAST-V, Longo Benedetto, Farcomeni Alessio, Ferri Germano, Campanale Antonella, Sorotos Micheal, Santanelli Fabio, Ovid Technologies (Wolters Kluwer Health), 2013
[31]
Breast Reduction, Hall-Findlay Elizabeth J., Shestak Kenneth C., Ovid Technologies (Wolters Kluwer Health), 2015
[32]
The Aesthetically Ideal Position of the Nipple–Areola Complex on the Breast, Lewin Richard, Amoroso Matteo, Plate Nikolina, Trogen Clara, Selvaggi Gennaro, Springer Science and Business Media LLC, 2016
[33]
The Aesthetically Ideal Position of the Nipple–Areola Complex on the Breast, Lewin Richard, Amoroso Matteo, Plate Nikolina, Trogen Clara, Selvaggi Gennaro, Springer Science and Business Media LLC, 2016
[34]
la correction du prolapsus mammaire . Le procédé de transposition du mamelon. , Passot R, Presse Med 1925;33:19, 1925
[35]
The no vertical scar breast reduction: A minor variation that allows to remove vertical scar portion of the inferior pedicle wise pattern T scar, Lalonde DH, Aesth Plast Surg 2003 27:335-344, 2003
[36]
A new technique for reduction mammaplasty, Ribeiro L, Plast Reconstr Surg, 1975
[37]
A new technique for reduction mammaplasty, Ribeiro L, Plast Reconstr Surg, 1975
[38]
Evidence-Based Medicine: Reduction Mammaplasty, Greco Richard, Noone Barrett, Ovid Technologies (Wolters Kluwer Health), 2017
[39]
Occult Pathologic Findings in Reduction Mammaplasty in 5781 Patients—An International Multicenter Study, Kuehlmann Britta, Vogl Florian D., Kempny Tomas, Djedovic Gabriel, Huemer Georg M., Hüttinger Philipp, Tinhofer Ines E., Hüttinger Nina, Steinstraesser Lars, Riml Stefan, Waldner Matthias, Bonham Clark Andrew, Schenck Thilo L., Wechselberger Gottfried, Haslik Werner, Koch Horst, Mandal Patrick, Rab Matthias, Pallua Norbert, Prantl Lukas, Larcher Lorenz, MDPI AG,
[40]
Evidence-Based Medicine: Reduction Mammaplasty, Greco Richard, Noone Barrett, Ovid Technologies (Wolters Kluwer Health), 2017
[41]
Evidence-Based Medicine, Kerrigan Carolyn L., Slezak Sheri S., Ovid Technologies (Wolters Kluwer Health), 2013
[42]
Venous Thromboembolism in Body Contouring, Wes Ari M., Wink Jason D., Kovach Stephen J., Fischer John P., Ovid Technologies (Wolters Kluwer Health), 2015
[43]
50 Shades of Red: The Predictive Value of Closed Suction Drains for the Detection of Postoperative Bleeding in Breast Surgery, Anker A. M., Miranda B. H., Prantl L., Kehrer A., Strauss C., Brébant V., Klein S. M., Springer Science and Business Media LLC, 2019