["4f04c199e5c38d73a1750acb5353956f81ffd8b8","42b4be201f4766cc48df2bfcdd9dcd3e1c4d6a61"]
Upper Arm Lift
brachioplasty
upper arm lift
body contouring
5943
5943
Chapter reads
0
0
Chapter likes
5/10
Evidence score
12
12
Images included
00
0
Videos included
01
Abstract
Abstract
Upper arm lifts are among the most complication-prone aesthetic procedures. In addition to hypertrophic and widened scarring, recurrences, wound dehiscence and wound infections must be expected in up to 40% of patients. Moreover the scar after an upper arm lift remains visible in everyday life at the cost of improved body contour.
The incision can be made medially (hidden scar position) or further dorsally (easier resection). In Regensburg we prefer a posterior-medial position, which is, in our opinion, the best compromise of both alternatives.
Depending on the tissue excess a limited, a standard horizontal or an extended L-shaped incision with an extension to the thoracic wall can be selected.
Liposuction is often necessary in addition to achieve the desired result.
02
Introduction
Introduction
Deformities of the upper arm occur due to the loss of skin elasticity as part of the aging process, due to weight fluctuations or after massive weight loss. The upper arm lift places high demands on the plastic surgeon, because, compared to other aesthetic procedures (e.g. abdominoplasty or breast reduction/augmentation), minor complications (e.g. hypertrophic and delayed or secondary wound healing) occur quite often (20-40 percent) and regardless of the surgical technique scares may be visible in the daily live. This must be into consideration in the context of informed consent.

hypertrophic scarring after a pure horizontal ellipsoid resection
Regarding the surgical approach a distinction must be made between an excess of fat, an excess of skin or a combination of both. While a pure excess of fat can be treated by liposuction alone, an excess of skin always requires tissue resection.
In addition, the location of the tissue excess plays a decisive role in the choice of therapy.
Pure proximal tissue excess can be sufficient addressed with a limited horizontal or a sole vertical incision
Tissue excess of the entire upper arm always requires a longer ellipsoid horizontal resection, possibly in combination with a vertical resection (T-shaped or fish-shaped incision).
If the tissue excess extends to the thorax (e.g. after massive weight loss), the incision should also extend to the thorax in a L-shaped pattern to address the tissue excess sufficient.
The position of the incision significantly influences the aesthetic result and the extent of the resection. A dorsal incision facilitates the resection in the area of the largest skin excess. However, a dorsal incision is clearly visible and therefore aesthetically problematic. In contrast a medial incision provides a hidden scar, but the skin-fat excess in the medial upper arm is only discretely pronounced. Consequently an adequate resection is only possible with a generous mobilization of the skin. Due to the skin tension after mobilization and the thin medial dermis, scars at the medial upper arm tend to widen and wound-healing disturbances are more often compared to the dorsal position.
An ideal classification and therapy algorithm of upper arm deformities was first published by Rohrich's working group in 1998 and modified in 2006. It takes into account all clinical characteristics and gives corresponding therapy recommendations for the individual clinical pictures.
03
Definition & Classification
Definition
Upper arm contouring can take the form of a tissue resection, liposuction or a combination of both techniques.The deformity is based on maasive weight loss, loss of skin elasticity due to the aging process and high weight fluctuations.
Classification
The working group around Rohrich et al. was able to update their classification, first published in 1998, again in 2006.Besides the high clinical relevance, a simple therapy algorithm can be derived from it.
Type
Skin Excess
Fat Excess
Location of Skin Excess
1
no
yes
2a
yes
no
proximal
2b
yes
no
entire arm
2c
yes
no
entire arm + chest
3a
yes
yes
proximal
3b
yes
yes
entire arm
3c
yes
yes
entire arm + chest
04
Algorithm
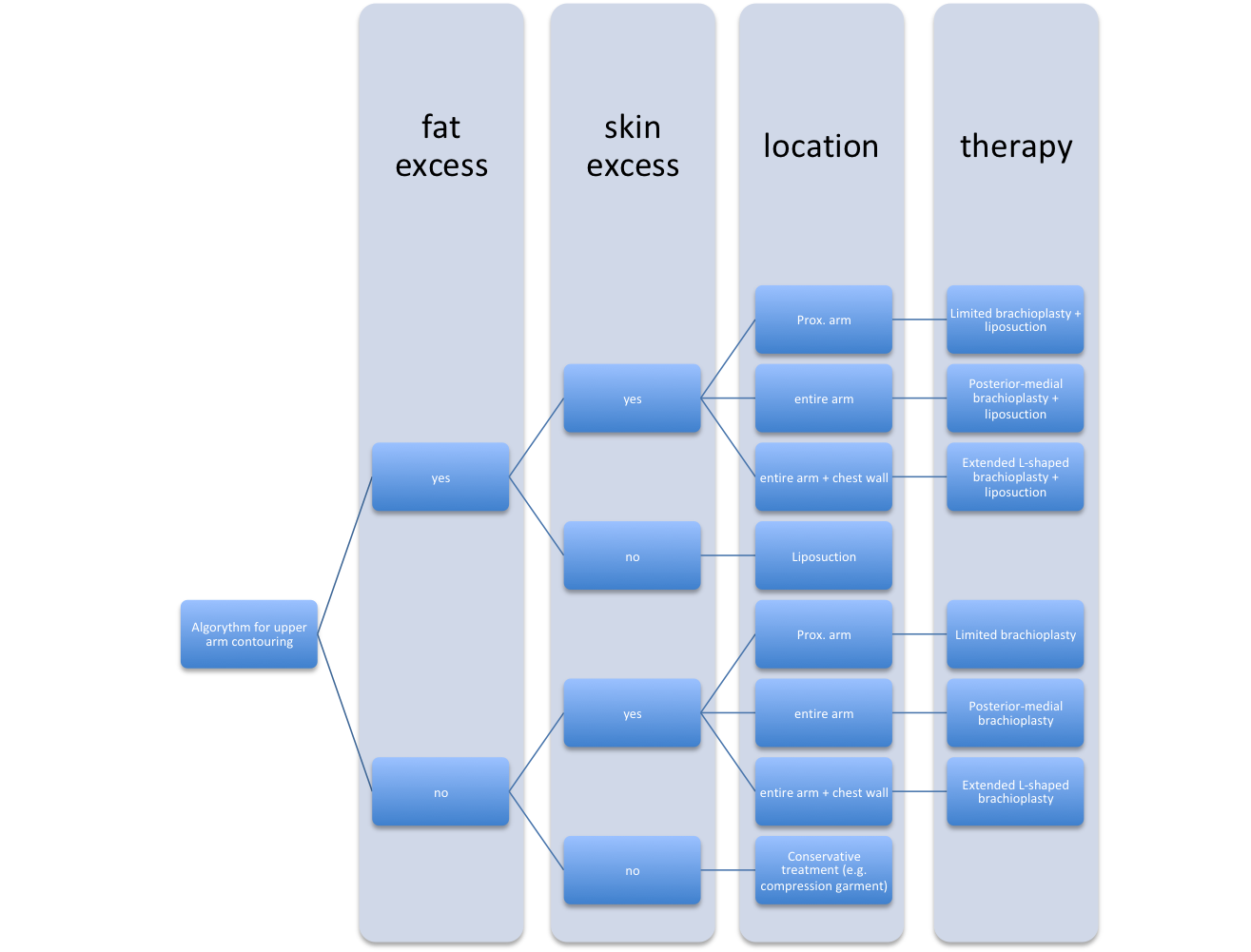
therapy algorithm adapted from Rohrich et al.
05
Anatomy
Anatomy
The skin of the upper arm is soft, elastic and very mobile. The dermis is clearly stronger dorsally than medially.
The superficial fascia surrounds the entire upper arm and its elasticity decreases in the aging process or after massive weight loss.
The deep fascia encloses the musculature as well as the relevant vascular-nerve structures and protects them from injury. To avoid serious complications, the deep upper arm fascia should never be injured during surgery.
Relevant fat rarely accumulates below the deep fascia and is predominantly localized in the dorsal upper arm. The effect of dorsal tissue excess is further enhanced by gravity-induced ptosis in the dorsal upper arm.
The relevant epifascial located structures that are in danger during dissection are the following sensitive nerves
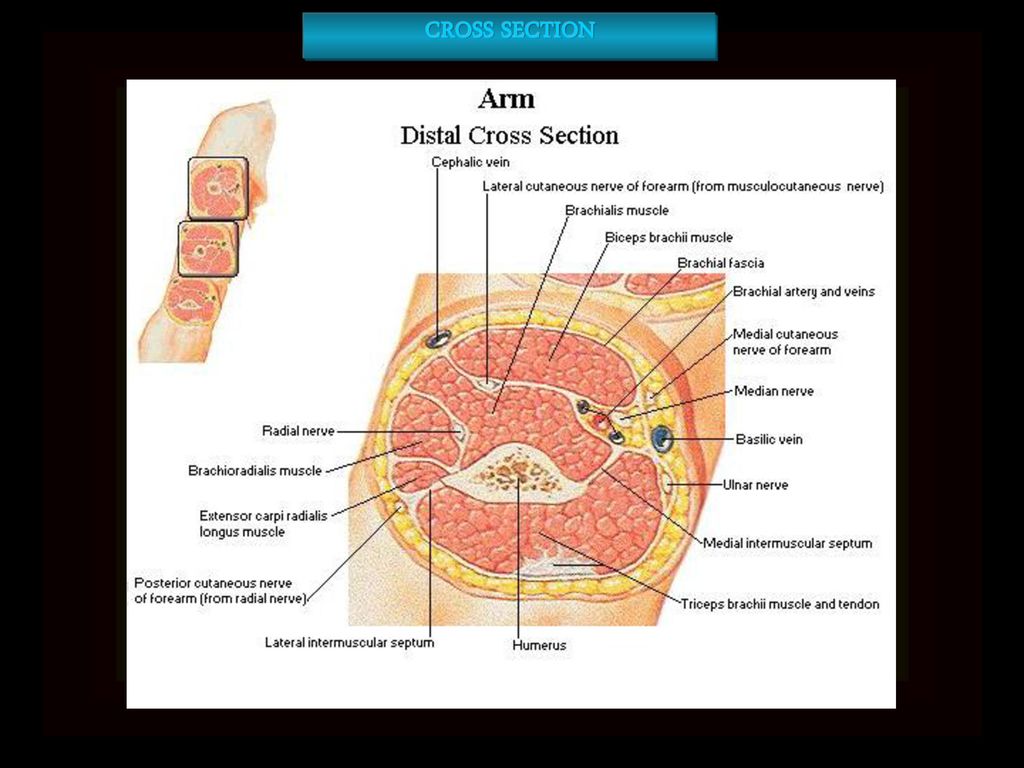
Cross section of the distal upper arm
the medial brachial cutaneous nerve
the medial antebrachial cutaneous nerve
the posterior brachial cutaneous nerve
the posterior antebrachial cutaneous nerve
And the following veins
cephalic vein
basilic vein
Despite the subfascial position, the ulnar nerve is in danger of iatrogenic injury at the medial epicondyle. As the subcutaneous tissue is very discrete in this area, violation of the nerve is possible especially during liposuction.
06
Preoperative planning
Preoperative planning
The following key points should be considered in the preoperative assessment
Exclusion of severe comorbidities (e.g. embolisms, thrombosis, lymphedema, dual anticoagulation).
Strict indication in case of relevant comorbidities (e.g. smokers, hypertrophic scarring in medical history), weight fluctuations, unrealistic expectations.
Exact recording and differentiation of the individual subtypes.
Preoperative markings
Preoperative markings should be done preoperatively on the awake patient with a waterproof pencil (shoulder 90° abducted; elbow 90° flexion). It has to be considered that disinfectants containing alcohol can remove the preoperative marking completely. On the other hand disinfectants containing iodine cause a distinct discoloration of the skin and require a longer drying phase.
Marking of a posterior-medial incision
There is controversy among plastic surgeons about the ideal position of the incision. While a medial localization can be better hidden in everyday life, wound-healing problems occur more often and resection is more difficult. In contrast tissue resection using a dorsal approach is easier and less prone to complications.
In Regensburg we prefer a posterior-medial incision described by Capella et al. or Chandawarkar et al. This position is the best compromise of both techniques. This approach conceals the later scar and at the same time allows adequate resection in the best possible way.
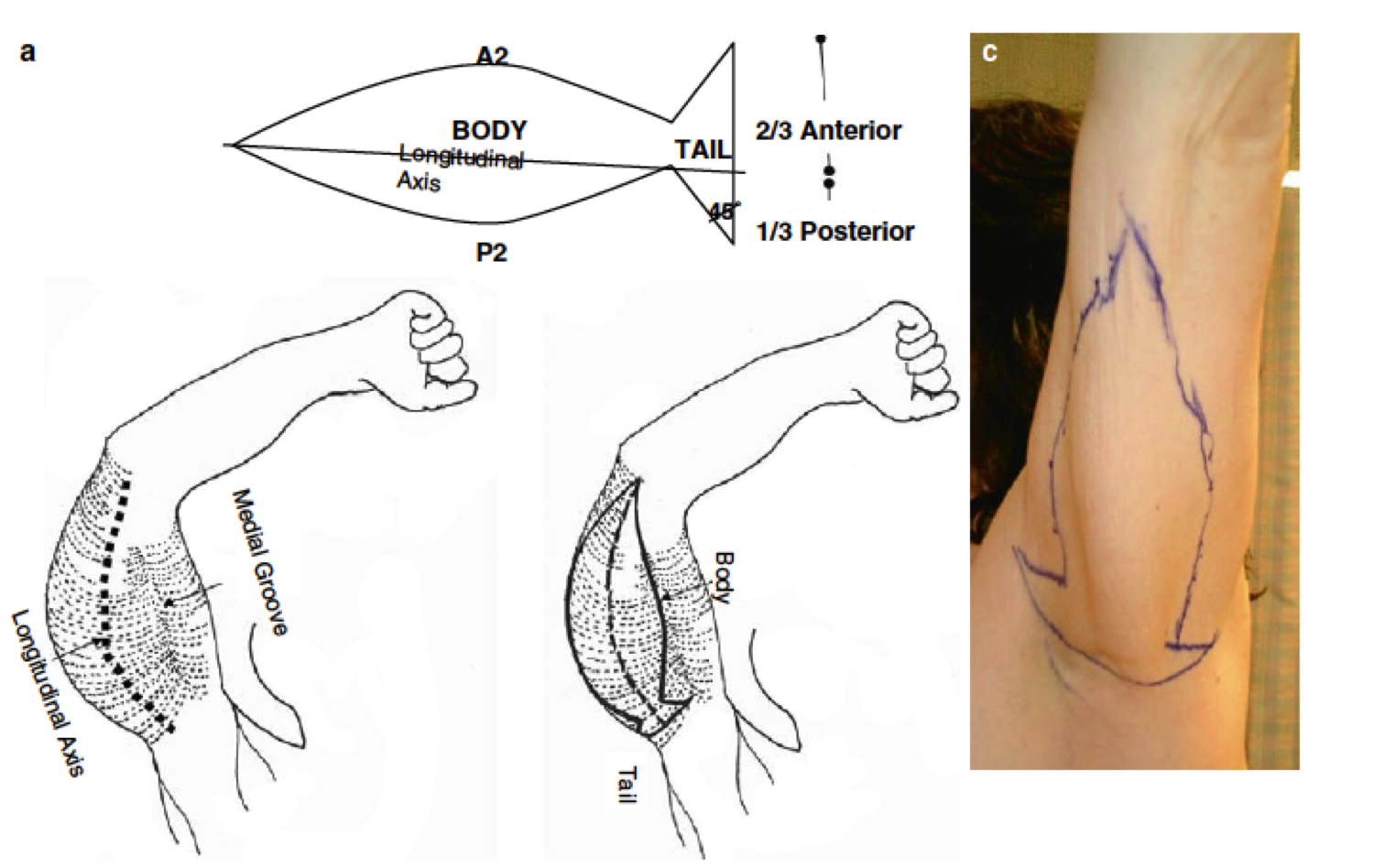
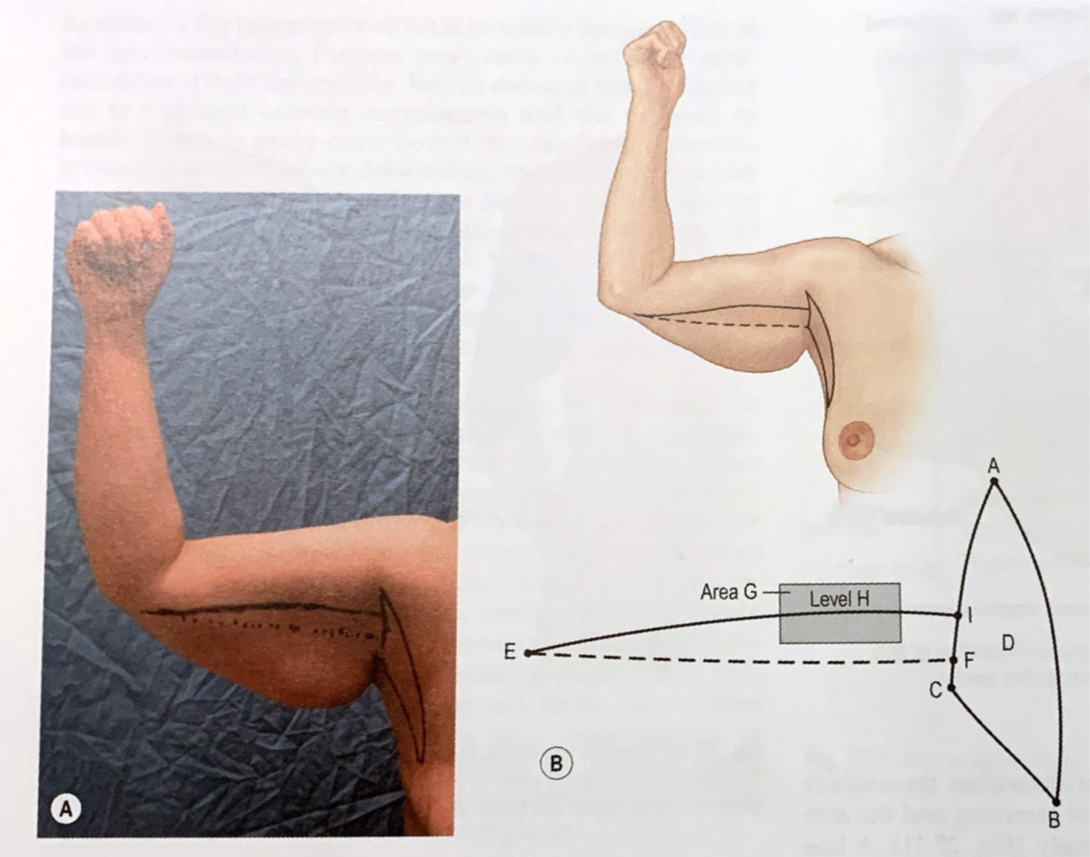
preoperative marking fish-shape resection adapted from Chandawarkar
A dotted line is drawn from the medial epicondyle to the axilla. The line runs a few (usually 3-4 cm) centimeters below and parallel to the bicipital groove over the triceps muscle. This line corresponds to the later scar position and to the axis of the resection figure.
Using a pinch test superior marking (corresponds to the upper resection) and inferior marking (corresponds to the lower resection) is estimated in an ellipsoid manner.
In order to ovoid over resection leading to vascular compromise and wound healing disturbance the double ellipse technique of Aly is recommended. This technique takes into account the amount of tissue between the surgeon’s fingers.
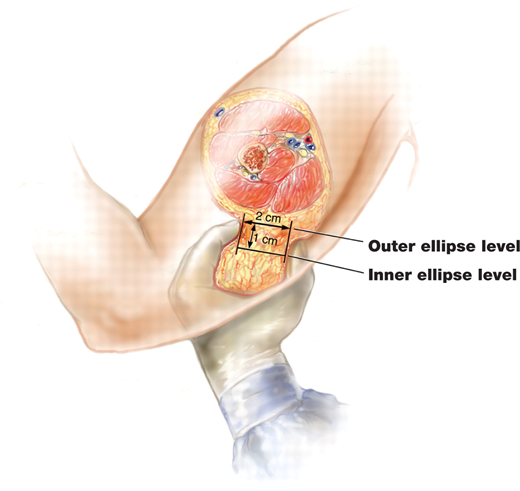
double ellipse technique adapted from Aly et al.
Outer ellipse is marked using the classic pinch-Test.
Inner ellipse (true incision) corresponds an additional inner marking half of the pinch thickness between the fingers.
Usually a fish-shaped (= t-shaped) resection, in addition to the ellipsoid resection figure is necessary to achieve an aesthetically pleasing result
A line is drawn from the lateral border of the pectoralis major muscle straight down to the anterior boarder of the latissimus dorsi muscle. This line corresponds to the vertical tail of the fish-shaped resection figure
.Connecting the upper and lower ends of this incision line with the horizontal ellipsis completes the fish-shaped resection figure.
The lower und upper part of the fish tail should form an angle of approximately 45°.
The upper and the lower part of the fish should be in the ratio of 2 thirds to 1 third.
Marking of an extended L-shaped posterior-medial incision
The marking of the upper arm is identical to points 1 and 2 of the posterior-medial incision. In addition to the ellipsoid marking of the upper arm, resection is carried out on the thorax
preoperative markings L-shape resection adapted from Neligan et al.
The first line is drawn from the upper medial end of the ellipsis to the lateral border of the pectoralis major muscle.
A second line is drawn along the lateral border of the pectoralis major muscle and extends to the thorax. The skin excess in the thoracic region determines the length of the incision.
A third line is drawn from along the anterior border of the latissimus dorsi muscle to the triceps muscle and the lower medial end of the ellipsis
The second and third line meet caudally and form an L-shaped resection figure.
Marking of a limited incision
A sole vertical ellipsoid resection figure in the axillary dome allows for tightening of a predominantly proximal, horizontal tissue excess and hides the scar as best as possible.
A lline connecting the lateral edge of the pectoris muscle and the anterior edge of the latissimus forms the vertical axis of the ellipsoidal resection figure.
A lline connecting the lateral edge of the pectoris muscle and the anterior edge of the latissimus forms the vertical axis of the ellipsoidal resection figure.
Alternatively, a small horizontal ellipsoidal resection with or without a fishtail analogue to a limited resection figure mentioned above can be useful for a combined vertical, horizontal and proximal tissue excess
07
Surgical technique
Surgical technique
In supine position both arms should be freely movable on an arm table. Even in pure upper arm lift or limited upper arm lift, at least the upper part of the thorax should be washed off.
The markings must be checked for completeness and redrawn if necessary. Orientation lines perpendicular to the incision should be drawn to ensure adequate wound edge adaptation after resection in order to avoid dog-ear configuration.
Frequent irrigation of the wound, bleeding or resection in combination with liposuction can wash away the orientation lines. Therefore the marking should be carried out far from the wound. Alternatively, temporary surgical staples could be placed to ensure subsequent alignment.
The extent of the resection should be reassessed and temporarily fixed with surgical staplers or clamps.
Final resection of the excess tissue can be performed in several steps to avoid overcorrection.
horizontal fish-shaped posterior-medial incision
The operation begins with incision of the superior marking of the horizontal ellipsis.
Epidermis and dermis is incised and dissected down to the deep fascia.
A skin/subcutaneous tissue flap is mobilized inferiorly.
Dissection is performed strict epifascial. Injury to the deep fascia must be avoided.
Hemostasis is consistently controlled with bipolar forceps or ligatures.
3-6 cm above the medial epicondyle the medial antebrachial cutaneous nerve and the basilica vein run superficial. Both structures literally stick on to the deep fascia and must be protected during the preparation.
After undermining and mobilizing the lower skin flap, it is pulled upwards with a towel clamp and thus the extent of the resection can be determined exactly.
The lower incision and thus the extent of resection is performed after setting the final amount of resection.
The lower incision should be planned conservatively. It may be reasonable to achieve the final resection only after repeated resection in order to avoid over-resection.
Before wound closure, a meticulous hemostasis must be performed. For this purpose the patient's blood pressure should be raised to a highly normal level.
Drains of size 10-12 gauge should be inserted through the axilla in order to prevent visible scaring of the drains.
Closure of the superficial fascia should be performed in order to avoid skin tension.
Subsequently adaptation of the dermis with subcutaneous sutures should be performed.
Skin closure is performed using absorbable suture material 3-0 or 4-0 monophilic intracutaneously continuous.

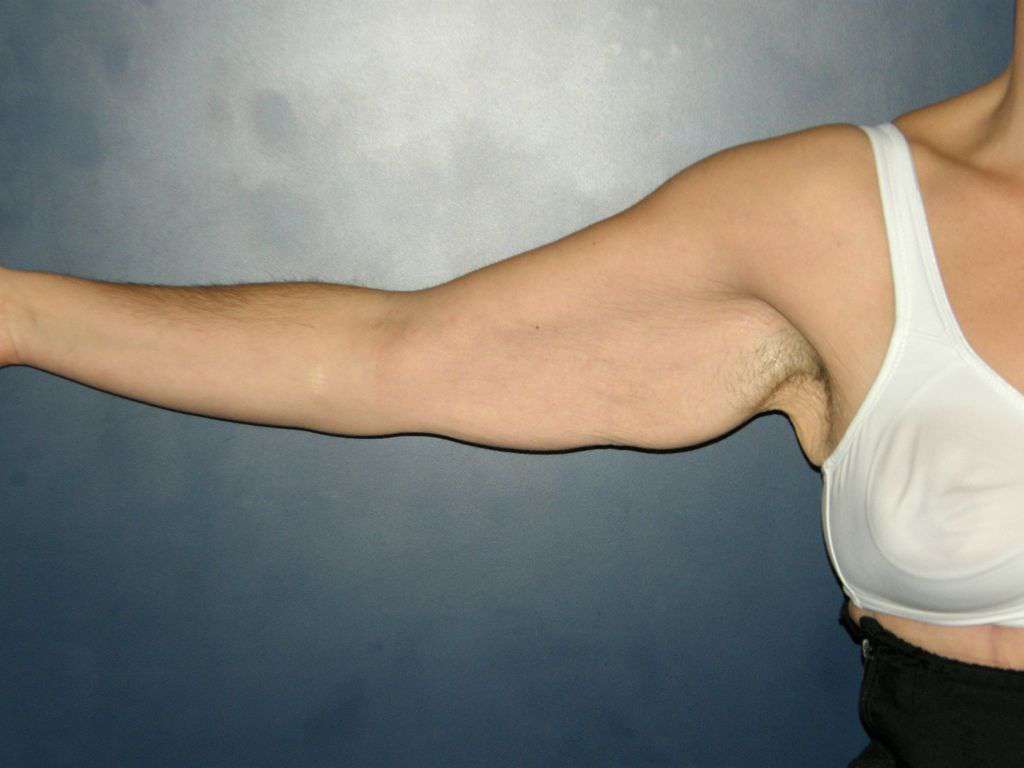
preoperative stage 2b

preoperative stage 2b flexed elbow

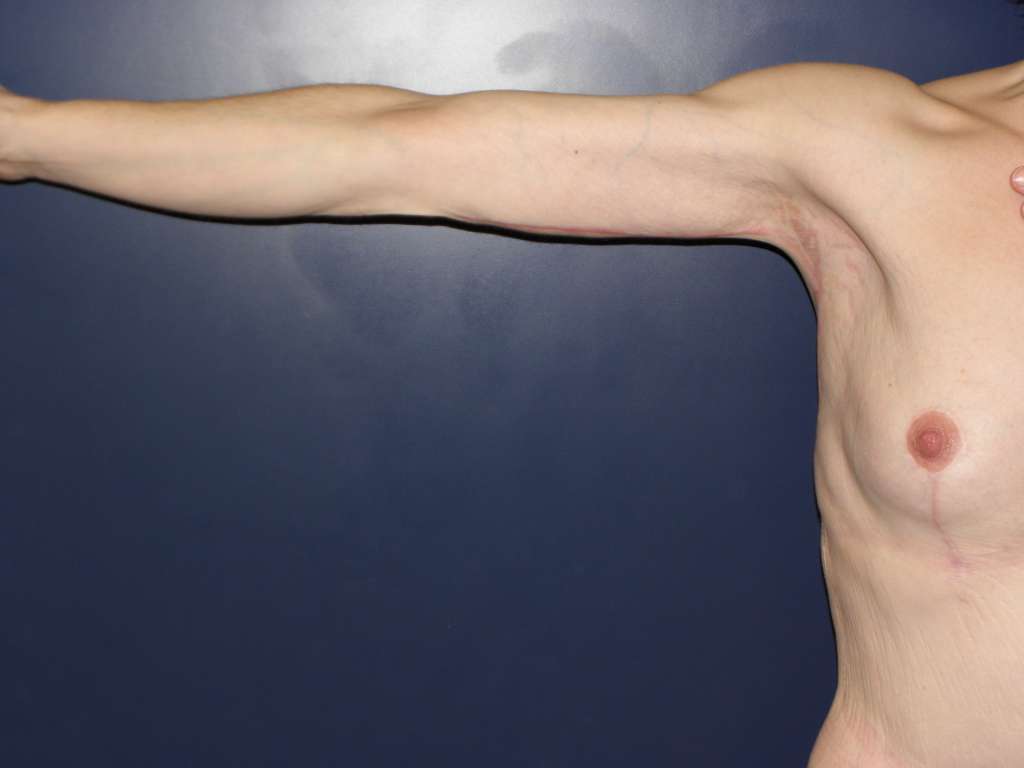
postoperative result after fish-shaped resection in a stage 2b deformity

postoperative result after fish-shaped resection in a stage 2b deformity
extended L-Shaped posterior-medial incision
In addition to the procedure of a horizontal resection. The resection is carried out to the thorax.
The amount of tissue resection should strictly follow the preoperative markings.
preoperative stage 2c
postoperative results after extended L-shaped resection of a stage 2c deformity
limited ellipsoid or t-shaped medial incision
Due to a pure horizontal and proximal localized tissue excess, a fishtail shaped resection in the axillary dome is sufficient.
For combined horizontal and vertical excess, a fish-shaped resection with a short horizontal leg is necessary.
The surgical technique is identical to the posterior-medial incision.
Liposuction
Liposuction can be performed as a two-stage procedure prior to brachioplasty or simultaneously
If liposuction is done simultaneously it should be done outside the incision to avoid excessive edema and tissue thinning.
Simultaneous liposuction allows for more precise shaping of the upper arm and a larger resection volume. However, the increased edema makes wound closure much more difficult and increases the risk of wound healing disorders.
Liposuction in close proximity to the medial epicondyle should be avoided to prevent uneventfully injury to the ulnar nerve.
08
Postoperative Care
Postoperative Care
Immediately after surgery, the upper arm should be wrapped elastically along with the thorax. As soon as possible, a custom-made compression garment should be fitted in order to prevent seromas.
First dressing change should be done at the 2nd postoperative day.
The amount of drainage should be checked regularly.
Before discharge and after removal of the drainage, a sonographic control should be performed to exclude a seroma
In case of a seroma, regular punctures (approx. every 2-3 days) should be performed under sonographic control.
09
Common complications
Common complications
Surgical pitfalls
Over resection and lack of possibility for primary wound closure
Injury of the medial antebrachial cutaneous nerve
Post-operative bleeding
Contractions in the axilla
General pitfalls
Too high expectations of the patient
Surgery in type 3 patients may lead to a disharmonious appearance between upper and lower arm (tightened upper arm vs. persisting excess fat around forearm)
Images
Cross section of the distal upper arm
double ellipse technique adapted from Aly et al.
preoperative markings L-shape resection adapted from Neligan et al.
preoperative marking fish-shape resection adapted from Chandawarkar
preoperative stage 2b
preoperative stage 2b flexed elbow
therapy algorithm adapted from Rohrich et al.
hypertrophic scarring after a pure horizontal ellipsoid resection
preoperative stage 2c
postoperative results after extended L-shaped resection of a stage 2c deformity
postoperative result after fish-shaped resection in a stage 2b deformity
postoperative result after fish-shaped resection in a stage 2b deformity
Videos
References
[1]
Plastic Surgery Volume two, Upper limb contouring, Joseph F Capella, Matthew J. Trovato, Scott Woehrle, J. Peter Rubin, Peter C Neligan, Elsevier, 2018
[2]
Body contouring, "Fish-incision" brachioplasty, Rajiv Y. Chandawarkar, Shiffman, Melvin A., DiGiuseppe, Alberto, Springer , 2010
[3]
The Constriction Arm Band Deformity in Brachioplasty Patients, Chen Wendy, James Isaac B., Gusenoff Jeffrey A., Rubin J. Peter, Ovid Technologies (Wolters Kluwer Health), 2018
[4]
Arm Contouring: Review and Current Concepts, Miotto Gabriele, Ortiz-Pomales Yan, Oxford University Press (OUP), 2018
[5]
Incidence and Risk Factors of Major Complications in Brachioplasty: Analysis of 2,294 Patients, Nguyen Lyly, Gupta Varun, Afshari Ashkan, Shack R. Bruce, Grotting James C., Higdon K. Kye, Oxford University Press (OUP), 2016
[6]
Body Contouring of the Arms and Brachioplasty, Hurwitz D., Neavin T., Georg Thieme Verlag KG, 2007
[7]
Upper Arm Contouring with Brachioplasty after Massive Weight Loss, Han Hyun Ho, Lee Min Cheol, Kim Sang Hwa, Lee Jung Ho, Ahn Sang Tae, Rhie Jong Won, Korean Society of Plastic and Reconstructive Surgeons, 2014
[8]
Long-Term Outcomes and Complications Associated with Brachioplasty: A Retrospective Review and Cadaveric Study, Knoetgen James, Moran Steven L., Ovid Technologies (Wolters Kluwer Health), 2006
[9]
Brachioplasty Outcomes, Zomerlei Terri A., Neaman Keith C., Armstrong Shannon D., Aitken Marguerite E., Cullen William T., Ford Ronald D., Renucci John D., VanderWoude Douglas L., Ovid Technologies (Wolters Kluwer Health), 2013
[10]
Liposuction-Assisted Short-Scar Brachioplasty, Hill Sean, Small Kevin H., Pezeshk Ronnie A., Rohrich Rod J., Ovid Technologies (Wolters Kluwer Health), 2016
[11]
Liposuction-Assisted Posterior Brachioplasty: Technical Refinements in Upper Arm Contouring, Nguyen Alexander T., Rohrich Rod J., Ovid Technologies (Wolters Kluwer Health), 2010
[12]
Liposuction-Assisted Medial Brachioplasty after Massive Weight Loss, de Runz Antoine, Colson Thomas, Minetti Christophe, Brix Muriel, Pujo Julien, Gisquet Heloïse, Simon Etienne, Ovid Technologies (Wolters Kluwer Health), 2015
[13]
An Algorithmic Approach to Upper Arm Contouring, Appelt Eric A., Janis Jeffrey E., Rohrich Rod J., Ovid Technologies (Wolters Kluwer Health), 2006
[14]
An Algorithmic Approach to Upper Arm Contouring, Appelt Eric A., Janis Jeffrey E., Rohrich Rod J., Ovid Technologies (Wolters Kluwer Health), 2006
[15]
An Algorithmic Approach to Upper Arm Contouring, Appelt Eric A., Janis Jeffrey E., Rohrich Rod J., Ovid Technologies (Wolters Kluwer Health), 2006
[16]
An Algorithmic Approach to Upper Arm Contouring, Appelt Eric A., Janis Jeffrey E., Rohrich Rod J., Ovid Technologies (Wolters Kluwer Health), 2006
[17]
Liposuction-Assisted Posterior Brachioplasty: Technical Refinements in Upper Arm Contouring, Nguyen Alexander T., Rohrich Rod J., Ovid Technologies (Wolters Kluwer Health), 2010
[18]
Liposuction-Assisted Medial Brachioplasty after Massive Weight Loss, de Runz Antoine, Colson Thomas, Minetti Christophe, Brix Muriel, Pujo Julien, Gisquet Heloïse, Simon Etienne, Ovid Technologies (Wolters Kluwer Health), 2015
[19]
Liposuction-Assisted Short-Scar Brachioplasty, Hill Sean, Small Kevin H., Pezeshk Ronnie A., Rohrich Rod J., Ovid Technologies (Wolters Kluwer Health), 2016
[20]
Incidence and Risk Factors of Major Complications in Brachioplasty: Analysis of 2,294 Patients, Nguyen Lyly, Gupta Varun, Afshari Ashkan, Shack R. Bruce, Grotting James C., Higdon K. Kye, Oxford University Press (OUP), 2016
[21]
Body contouring, "Fish-incision" brachioplasty, Rajiv Y. Chandawarkar, Shiffman, Melvin A., DiGiuseppe, Alberto, Springer , 2010
[22]
Plastic Surgery Volume two, Upper limb contouring, Joseph F Capella, Matthew J. Trovato, Scott Woehrle, J. Peter Rubin, Peter C Neligan, Elsevier, 2018
[23]
Brachioplasty After Massive Weight Loss: A Simple Algorithm for Surgical Plane, Cannistra Claudio, Valero Rodrigo, Benelli Charles, Marmuse Jean Pierre, Springer Science and Business Media LLC, 2007
[24]
Body contouring, "Fish-incision" brachioplasty, Rajiv Y. Chandawarkar, Shiffman, Melvin A., DiGiuseppe, Alberto, Springer , 2010
[25]
Modified Fish-Incision Technique in Brachioplasty: A Surgical Approach to Correct Excess Skin and Fat of the Upper Arm (Restoring the Armpit Contour), Ferraro Giuseppe A., De Francesco Francesco, Razzano Sergio, D’Andrea Francesco, Nicoletti Gianfranco, Springer Science and Business Media LLC, 2015
[26]
The L Brachioplasty: An Innovative Approach to Correct Excess Tissue of the Upper Arm, Axilla, and Lateral Chest, Hurwitz Dennis J., Holland Sarah W., Ovid Technologies (Wolters Kluwer Health), 2006
[27]
The Constriction Arm Band Deformity in Brachioplasty Patients, Chen Wendy, James Isaac B., Gusenoff Jeffrey A., Rubin J. Peter, Ovid Technologies (Wolters Kluwer Health), 2018