["b5253982ad925e2c131e35dfc76354bd43d1d52e"]
Wrist denervation
wrist
denervation
pain
hand
arthrosis
2562
2562
Chapter reads
0
0
Chapter likes
4/10
Evidence score
03
3
Images included
00
0
Videos included
01
Introduction
Introduction
Wrist denervation, a surgical intervention employed to manage persistent wrist pain, is both safe and efficient, potentially averting or postponing the need for more invasive, kinematics-altering salvage procedures. Since its initial description in 1959, the popularity of wrist denervation has been on an upward trajectory, with the procedure evolving from more extensive denervations to simplified single-incision techniques. In the management of chronic wrist pain, numerous practitioners have utilized this technique not only as a palliative treatment but also as a supplementary approach alongside other surgical interventions.2
02
Anatomy
Anatomy
Median Nerve: The median nerve doesn't directly supply any known articular branches as it traverses across the wrist into the carpal tunnel. It provides innervation to the joint through its Anterior Interosseous Nerve (AIN) and palmar cutaneous nerve branches.
Ulnar Nerve: The ulnar nerve supplies the ulnar side of the wrist through a branch arising from the dorsal sensory ulnar nerve, as well as branches from the deep motor branch of the ulnar nerve. This deep motor branch is situated near the hook of the hamate. Additional smaller articular branches permeate the intermetacarpal spaces, and they emerge on the dorsal aspect to supply the carpometacarpal joints from the index to the small fingers.
Radial Nerve: The radial nerve provides innervation to the wrist joint via the Posterior Interosseous Nerve (PIN) and minor branches originating from the radial sensory nerve. Other relevant nerves in this location include the Lateral Antebrachial Cutaneous Nerve (LABCN), which is found running longitudinally, accompanying the radial artery. Also, minor branches from the posterior and medial antebrachial cutaneous nerves may offer articular innervation.1
Ulnar Nerve: The ulnar nerve supplies the ulnar side of the wrist through a branch arising from the dorsal sensory ulnar nerve, as well as branches from the deep motor branch of the ulnar nerve. This deep motor branch is situated near the hook of the hamate. Additional smaller articular branches permeate the intermetacarpal spaces, and they emerge on the dorsal aspect to supply the carpometacarpal joints from the index to the small fingers.
Radial Nerve: The radial nerve provides innervation to the wrist joint via the Posterior Interosseous Nerve (PIN) and minor branches originating from the radial sensory nerve. Other relevant nerves in this location include the Lateral Antebrachial Cutaneous Nerve (LABCN), which is found running longitudinally, accompanying the radial artery. Also, minor branches from the posterior and medial antebrachial cutaneous nerves may offer articular innervation.1

Neuroanatomy
AIN = anterior interosseous nerve, DSBUN = dorsal sensory branch of the ulnar nerve, FCR = flexor carpi radialis, LABCN = lateral antebrachial cutaneous nerve, PIN = posterior interosseous nerve, SBRN = superficial branch of radial nerve1
03
Indication
Indication
The perfect candidate for this procedure would be an individual who has reached skeletal maturity and is suffering from a chronic, painful condition affecting the radiocarpal or ulnocarpal areas of the wrist. Such individual would have endured significant wrist pain, warranting a surgical intervention, despite having attempted all conservative treatments.
The aim of wrist denervation is to provide long-term pain relief and improve function while avoiding more aggressive procedures,that may lead to significant alterations in wrist mechanics and function.
- Chronic wrist pain: The primary indication for wrist denervation is chronic wrist pain, especially when pain is diffuse, constant, and significantly affects the patient's quality of life
- Post-Traumatic arthrosis: persistent pain despite conservative treatments,
- Scapholunate Advanced Collapse (SLAC) and Scaphoid Nonunion Advanced Collapse (SNAC): when conservative treatments fail
- Kienbock's disease: In certain stages of Kienbock's disease, wrist denervation can be employed to alleviate pain
In addition, adolescents requiring surgery for Kienbock disease may also benefit from concomitant denervation.
Adjunct to Other Procedures: Wrist denervation can also be performed in conjunction with other surgical procedures, such as partial wrist fusion, proximal row carpectomy, or wrist arthroplasty, to enhance pain relief 1
The aim of wrist denervation is to provide long-term pain relief and improve function while avoiding more aggressive procedures,that may lead to significant alterations in wrist mechanics and function.
- Chronic wrist pain: The primary indication for wrist denervation is chronic wrist pain, especially when pain is diffuse, constant, and significantly affects the patient's quality of life
- Post-Traumatic arthrosis: persistent pain despite conservative treatments,
- Scapholunate Advanced Collapse (SLAC) and Scaphoid Nonunion Advanced Collapse (SNAC): when conservative treatments fail
- Kienbock's disease: In certain stages of Kienbock's disease, wrist denervation can be employed to alleviate pain
In addition, adolescents requiring surgery for Kienbock disease may also benefit from concomitant denervation.
Adjunct to Other Procedures: Wrist denervation can also be performed in conjunction with other surgical procedures, such as partial wrist fusion, proximal row carpectomy, or wrist arthroplasty, to enhance pain relief 1
04
Algorythm
Algorythm
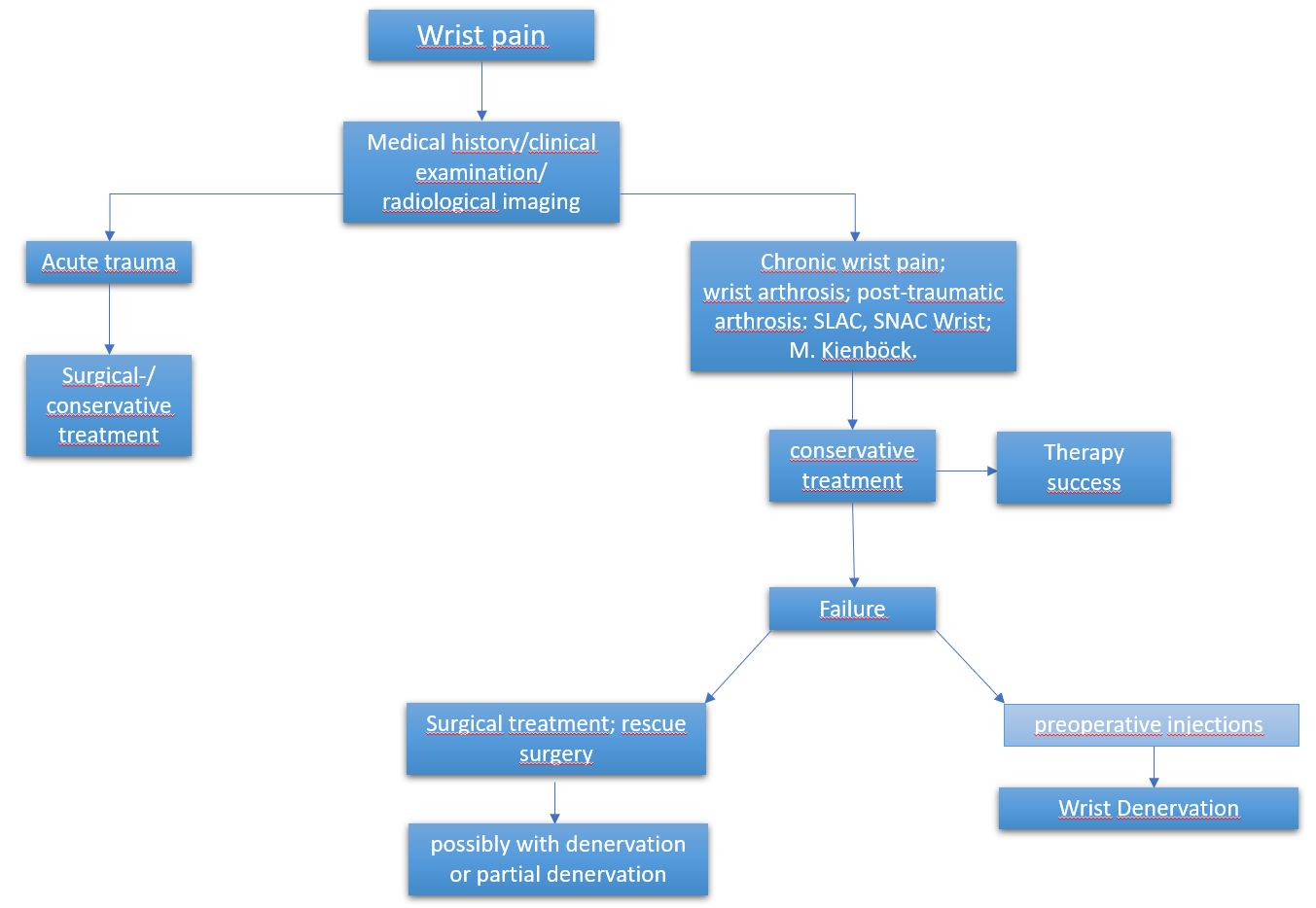
Wrist denervation algorhythm
05
Preoperative test
Preoperative test
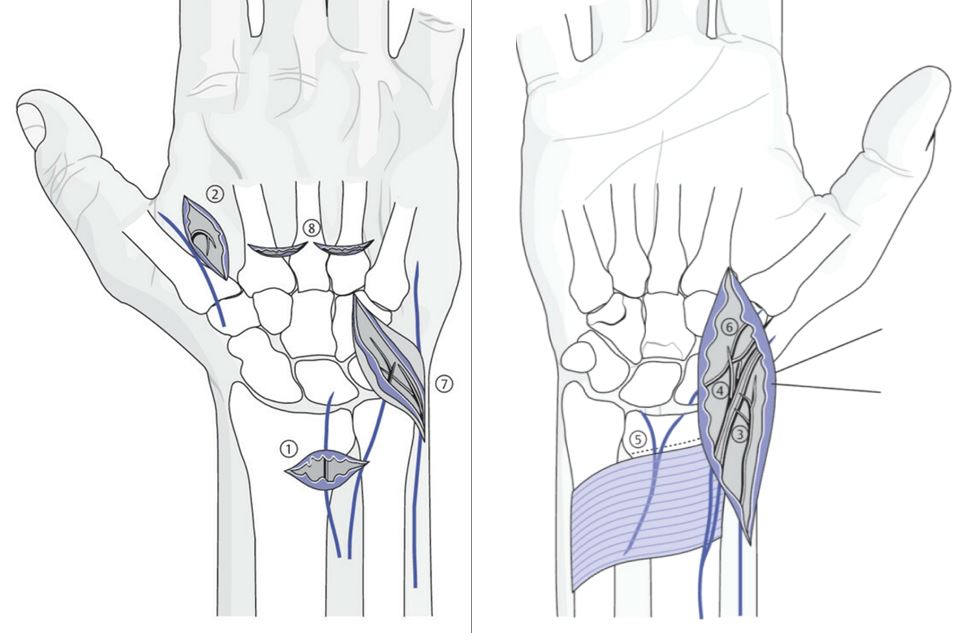
1. Posterior interosseous nerve (PIN): dorsomedian injection perpendicular, about 3 cm proximal to the carpus to the radius.
2. Articular Branch of the First Interosseous Space: subcutaneous depot dorsally between the base of the first and second metacarpal bones at the ulnar edge of the often clearly visible first intermetacarpal vein.
3. R. superficialis n. radialis: this requires a transversely applied subcutaneous infiltration.
4. Articular branches of the N. cutaneus antebrachii lateralis: paravasal depot of 1 ccm local anesthetic in the area of the radial vessels about 3 cm proximal to the carpus.
5. Anterior Interosseous Nerve (AIN): ventromedian puncture perpendicular, about 3 cm proximal to the rascetta, on the ulnar edge of the Palmaris Longus muscle; local anesthetic depot directly over the radius and the interosseous membrane.
6. R. palmaris n. medianus: Subcutaneous infiltration between the radial artery and the tendons of the Palmaris Longus muscle.
7. R. dorsalis n. ulnaris and the articular branches of the antebrachial cutaneous nerves (variations): puncture on the ulnar side of the PSU and extensive infiltration to the bone as well as to the volar.
8. Perforating Branches II and III: a small local anesthetic depot dorsally directly over the corresponding intermetacarpal joints.3
2. Articular Branch of the First Interosseous Space: subcutaneous depot dorsally between the base of the first and second metacarpal bones at the ulnar edge of the often clearly visible first intermetacarpal vein.
3. R. superficialis n. radialis: this requires a transversely applied subcutaneous infiltration.
4. Articular branches of the N. cutaneus antebrachii lateralis: paravasal depot of 1 ccm local anesthetic in the area of the radial vessels about 3 cm proximal to the carpus.
5. Anterior Interosseous Nerve (AIN): ventromedian puncture perpendicular, about 3 cm proximal to the rascetta, on the ulnar edge of the Palmaris Longus muscle; local anesthetic depot directly over the radius and the interosseous membrane.
6. R. palmaris n. medianus: Subcutaneous infiltration between the radial artery and the tendons of the Palmaris Longus muscle.
7. R. dorsalis n. ulnaris and the articular branches of the antebrachial cutaneous nerves (variations): puncture on the ulnar side of the PSU and extensive infiltration to the bone as well as to the volar.
8. Perforating Branches II and III: a small local anesthetic depot dorsally directly over the corresponding intermetacarpal joints.3
06
Surgical technique according to Wilhelm
Surgical technique according to Wilhelm
Surgical technique according to Wilhelm
1 Exposure posterior interosseous nerve (PIN) from a transverse incision 3 cm proximal to the carpus (finger extensor tendons are held ulnar). If possible proximal transection, grasp proximal nerve stump and tear out.
2. Expose R. articularis spatii interossei I from small skin incision above the first intermetacarpal joint (near the division point of the radial branch running to D1 and D2, which is accompanied dorsoradially by a vein and runs to palmar).
3. On the radial flexion side, a skin incision extending from the trapezium to above pron. quadratus is made. Epifascial dissection of the skin mantle around the dist. radius and PSR in a dorsal direction: separation of the articular branches that run from the R. superficial n. radialis in the subcutis.
4. Elimination of the terminal branches of the N. cutaneus antebrachii lateralis running to the joint via the same skin incision after exposure of the radial artery by ligating and cutting through the extra-paraval tissue.
5. Exposure of the pron. quadratus between the radial artery and the FCR tendon, holding the flexor tendons ulnar, cutting the connective tissue at the distal radius electrically down to the periosteum parallel to the articular surface together with the nerves therein to interrupt the anterior interosseous nerve (AIN).
6. Subcutaneous dissection medially to cut the end branches of the R. palmaris n. mediani.
7. If the pain symptomatology extends to the ulnar wrist: slightly S-shaped curved cut dorsoulnar, epifascial dissection of the skin around PSU and ulnar wrist (articular branches N. ulnaris, while sparing the subcutaneously running R. dorsalis n. ulnaris; N. cut. antebr. post., N. cut. antebr. med.
8. In case of pain in distal carpal row: Dorsal exposure of the intercarpal joints II and III (transverse skin incision, keeping the extensor tendons apart), electrical transection of the nerve-containing connective tissue above the base of the MHKs3
2. Expose R. articularis spatii interossei I from small skin incision above the first intermetacarpal joint (near the division point of the radial branch running to D1 and D2, which is accompanied dorsoradially by a vein and runs to palmar).
3. On the radial flexion side, a skin incision extending from the trapezium to above pron. quadratus is made. Epifascial dissection of the skin mantle around the dist. radius and PSR in a dorsal direction: separation of the articular branches that run from the R. superficial n. radialis in the subcutis.
4. Elimination of the terminal branches of the N. cutaneus antebrachii lateralis running to the joint via the same skin incision after exposure of the radial artery by ligating and cutting through the extra-paraval tissue.
5. Exposure of the pron. quadratus between the radial artery and the FCR tendon, holding the flexor tendons ulnar, cutting the connective tissue at the distal radius electrically down to the periosteum parallel to the articular surface together with the nerves therein to interrupt the anterior interosseous nerve (AIN).
6. Subcutaneous dissection medially to cut the end branches of the R. palmaris n. mediani.
7. If the pain symptomatology extends to the ulnar wrist: slightly S-shaped curved cut dorsoulnar, epifascial dissection of the skin around PSU and ulnar wrist (articular branches N. ulnaris, while sparing the subcutaneously running R. dorsalis n. ulnaris; N. cut. antebr. post., N. cut. antebr. med.
8. In case of pain in distal carpal row: Dorsal exposure of the intercarpal joints II and III (transverse skin incision, keeping the extensor tendons apart), electrical transection of the nerve-containing connective tissue above the base of the MHKs3
07
Postoperative care
Postoparative care
- Wrist splint for one month
- After safe wound healing, the splint can be removed for showering
- Immediate movement of the fingers
- Patients should be informed that the volar incision may be painful for several monthsand that the full benefit of the operationmay not be fully realized until after 6 months.1
- After safe wound healing, the splint can be removed for showering
- Immediate movement of the fingers
- Patients should be informed that the volar incision may be painful for several monthsand that the full benefit of the operationmay not be fully realized until after 6 months.1
08
Recommendation
Recommendation
A limited denervation approach that targets the Anterior Interosseous Nerve (AIN), the Posterior Interosseous Nerve (PIN), branches of the Lateral Antebrachial Cutaneous Nerve (LABCN), and the Superficial Branch of the Radial Nerve (SBRN) has proven satisfactory for most patients.
The pain relief resulting from an isolated Posterior Interosseous Nerve (PIN) neurectomy tends to diminish over time, especially when compared to the sustained effectiveness of the traditional Wilhelm denervation procedure.
Denervation of the Posterior Interosseous Nerve (PIN) can effectively reduce dorsal wrist pain.
Patients should be advised that this procedure should achieve pain relief of approximately 80%. Advantage of this procedure is that the mobility is preserved. however, the possibility of future more definitive rescue measures is not excluded.
It is controversial whether the success of preoperative injections can be a reliable indicator of the degree of postoperative pain relief.1
The pain relief resulting from an isolated Posterior Interosseous Nerve (PIN) neurectomy tends to diminish over time, especially when compared to the sustained effectiveness of the traditional Wilhelm denervation procedure.
Denervation of the Posterior Interosseous Nerve (PIN) can effectively reduce dorsal wrist pain.
Patients should be advised that this procedure should achieve pain relief of approximately 80%. Advantage of this procedure is that the mobility is preserved. however, the possibility of future more definitive rescue measures is not excluded.
It is controversial whether the success of preoperative injections can be a reliable indicator of the degree of postoperative pain relief.1
Videos
References
[1]
Denervation of the Wrist Joint for the Management of Chronic Pain, Kadiyala RK, Lombardi JM, J Am Acad Orthop Surg, 2017
[2]
Wrist Denervation, Wu Chia H., Strauch Robert J., Elsevier BV, 2019
[3]
Wrist Denervation, Wu Chia H., Strauch Robert J., Elsevier BV, 2019
[4]
Wrist Denervation, Wu Chia H., Strauch Robert J., Elsevier BV, 2019
[5]
Die Denervierung des Handgelenkes — Anatomie, operative Technik, Indikation, Grechenig W., Tesch N. P., Mähring M., Springer Science and Business Media LLC, 2002
[6]
Die Denervierung des Handgelenkes — Anatomie, operative Technik, Indikation, Grechenig W., Tesch N. P., Mähring M., Springer Science and Business Media LLC, 2002
[7]
Wrist Denervation, Wu Chia H., Strauch Robert J., Elsevier BV, 2019
[8]
Wrist Denervation, Wu Chia H., Strauch Robert J., Elsevier BV, 2019